
There are few systems that can efficiently incorporate materials that provide structural support, filtration capacity, energy generation, energy storage, electrical conductivity, gas exchange, processing power, dynamic flexibility, and regenerative potential into one integrated, highly functional, and incredibly adaptable self-contained system.
Yet the human body is a system that can provide all those functions and many more, and it does so through a unique collection of highly functional materials.
Collectively those materials enable everything our bodies do, and they often retain functionality throughout the human lifespan, which worldwide is an average of 73.2 years.1 However, the materials are not always perfect and sometimes fail due to overuse, injury, disease, or genetics—circumstances that are becoming more common as worldwide populations age due to population dynamics and increasing life expectancies.
Globally, the number of individuals over 65 years old surpassed that of children under 5 years old for the first time in history in 2018. And while an estimated one in 11 individuals (9%) around the world were over 65 years old in 2019, the older population is expected to increase to one in six (16%) by 2050.2
These trends affect nearly every aspect of life, perhaps most notably healthcare. Individuals are living longer and are remaining active until later years of life, demanding enhanced strategies to maintain longer functionality of the body’s materials.
Humans have long turned to biomaterials in diverse forms to repair, replace, or enhance bodily materials (Figure 1), establishing a global market for implantable biomaterials that was estimated to be worth nearly $110 billion in 2019.3 While metals, polymers, ceramics, and glass all are used for biomaterial applications, ceramics and glass have a particular advantage, says Frank Anderson, vice president of Global Research and Development at CoorsTek (Golden, Colo.). “Many technical ceramics are inherently biocompatible, chemically-resistant, and inert, which gives them a unique advantage over other implantable materials,” he says.
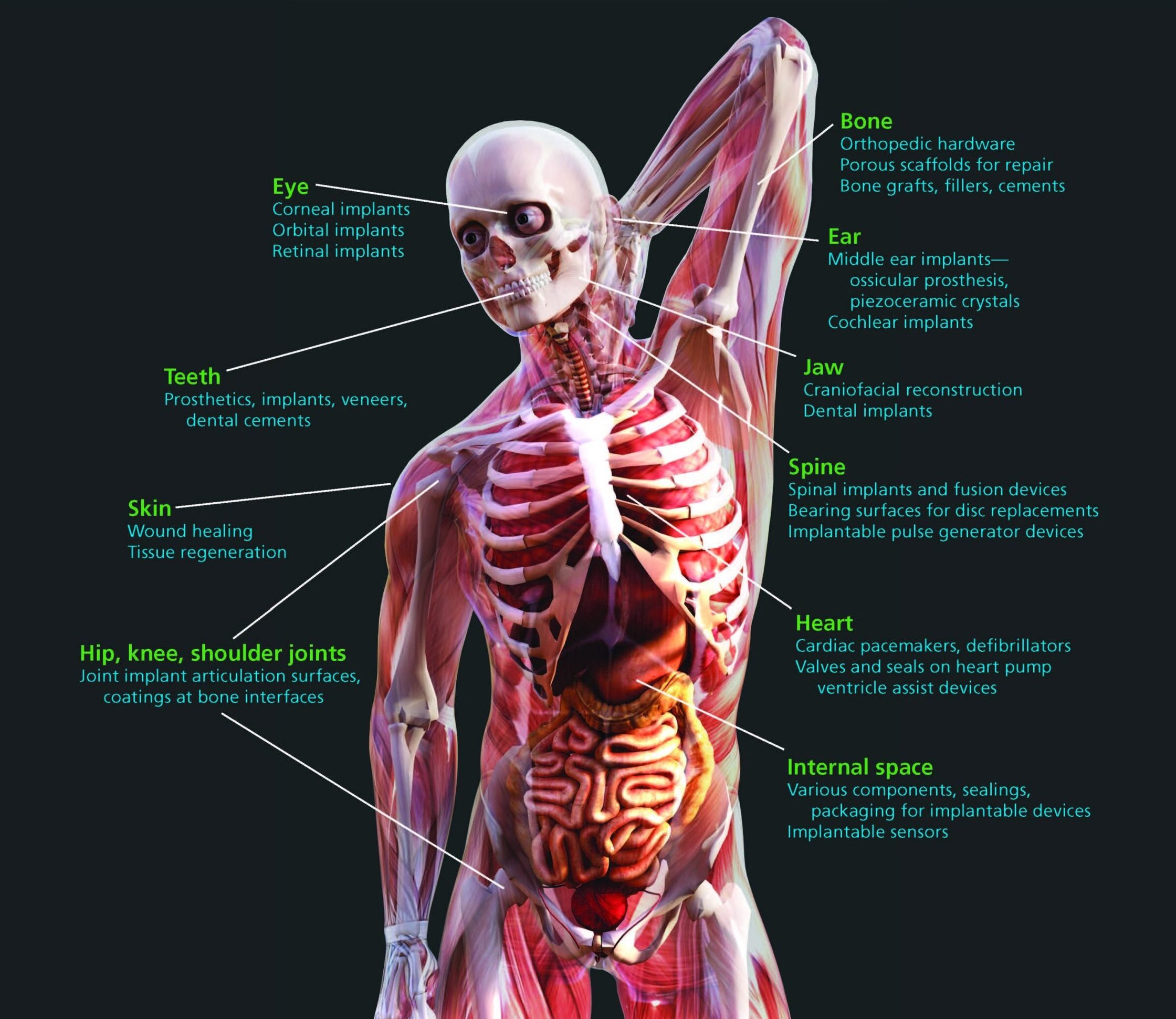
Figure 1. Ceramics and glass help repair, replace, and enhance all types of bodily materials. Background image credit: iStock.com/mrjo2405
The global market for bioceramics was valued at $14.5 billion in 2016 and is predicted to reach a value of $20.2 billion by 2021, growing at a 6.9% compound annual growth rate (CAGR).4 The market is mainly dominated by alumina and zirconia, which account for 75% of the market due to primary use of these materials in bone and dental implants. Other bioceramics frequently found in implantable devices include hydroxyapatite and tricalcium phosphate, and bioactive glass also has clinical applications with rapidly expanding potential throughout the human body.
It should be noted that while these materials predominate many implantable applications within the human body, mainly due to their acceptance and time on the market, other ceramic and glass compositions are also suitable for many of these applications, and we might expect their purview to expand in future markets.
Collectively, ceramic and glass materials enable many different kinds of implantable medical products that not only significantly contribute to human health but also constitute robust industries with rich economic impact. Table 1 provides a sample of some companies that manufacture ceramic and glass biomaterials or implantable products.
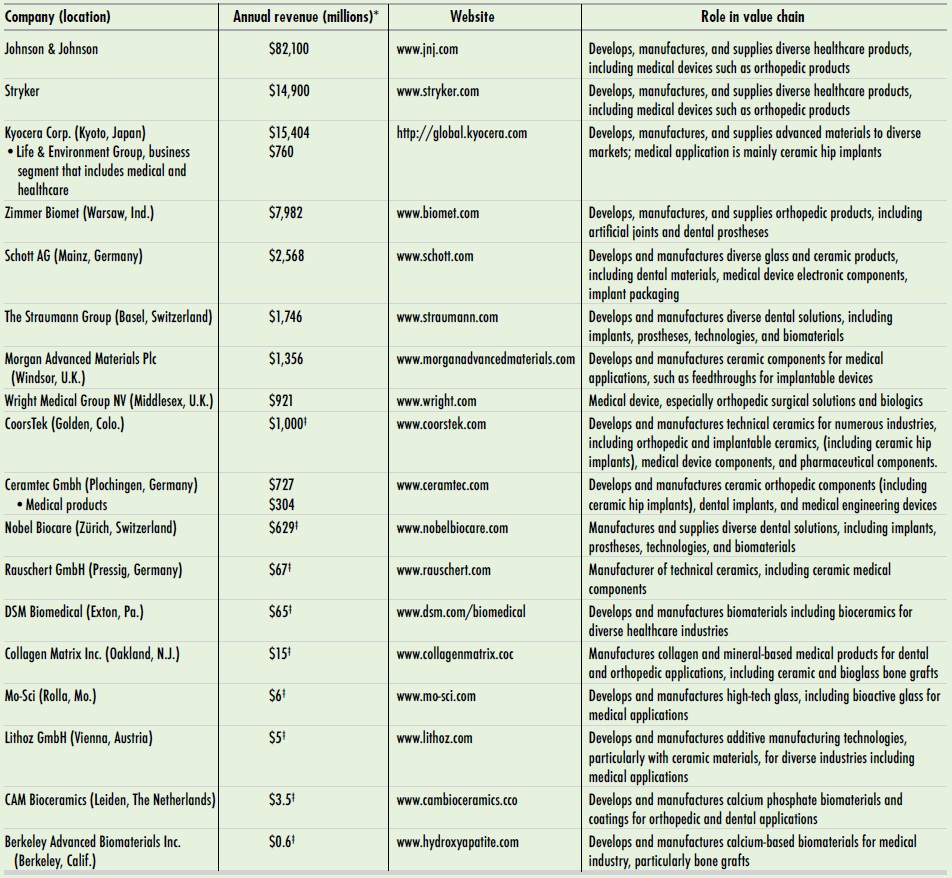
Table 1. Select companies that manufacture ceramic and glass implantable medical products or components* *Conversions per Google as of October 16, 2020. All financial data obtained from company reports unless otherwise noted. ‡Private company or data not available; revenue estimated from dnb.com or google.com.
The following sections highlight a handful of applications for ceramics and glass in the human body. Although the listed applications are not exhaustive, the diversity highlighted here should provide a flavor of the vast potential of ceramics and glass within the human body.
Packaging: Glass protects both body and device
Ceramic and glass materials are incorporated into or play supporting roles in many electronic devices implanted into the human body, such as neurostimulators and pacemakers. In these applications, a bioinert and long-lasting barrier between the device components and the harsh environment of the body is imperative to protect both—precisely a job for ceramics and glass.
For instance, glass-sealed feedthroughs and packaging often encase the batteries for implantable pacemakers, where a hermetic seal preserves both function of the device and safety of the patient.
“Glass is used to seal the terminals of pacemaker batteries. It acts as an electrical insulation material for the metal conductors. At the same time, glass creates a reliably gas-tight barrier when hermetically sealed with the electrical contact pins,” says Jochen Herzberg, medical program manager of Schott’s Electronic Packaging business unit (Landshut, Germany). “Specially selected glass types are resistant to the highly corrosive environment in the battery. And it doesn’t deteriorate or get brittle over time like polymers or epoxies. It enables a higher reliability and a longer device lifetime.”
To manufacture the glass-to-metal sealed packages and feedthroughs, Schott presses finely ground glass powder into a ring shape that is then sintered and assembled with the metal conductors inserted in the middle of the ring and an outer metal casing. The three components then undergo a sealing process in a belt furnace to bond the materials together.
Although this manufacturing technique provides a hermetic seal for battery feedthroughs, there is another glass technology that comes into play when miniaturization or encapsulation of heat-sensitive components is required. For those applications, Schott has another solution with its Primoceler glass micro-bonding technology. This wafer-scale technology uses a laser to precisely and locally bond glass to glass, creating a vacuum-tight bond with no additional materials.
“If you want to encapsulate, for example, a miniature sensor inside of a glass package, this is possible by stacking base wafers with spacer glass and cover or etched lid wafers, thereby creating a cavity in which the sensor device will be encapsulated,” Herzberg says. “The stacked glass wafers are then laser-sealed, resulting in a gas-tight all-glass sensor package. One major advantage of Primoceler laser bonding technology is that it all happens at room temperature. So even if the sensor is very heat sensitive, which is usually the case, it can be packaged using the Schott Primoceler process. The extremely precise laser fuses and melts only the very small interface area where the glass wafers meet—an area of just some tens of microns—while leaving all other surfaces untouched.” (Figure 2)
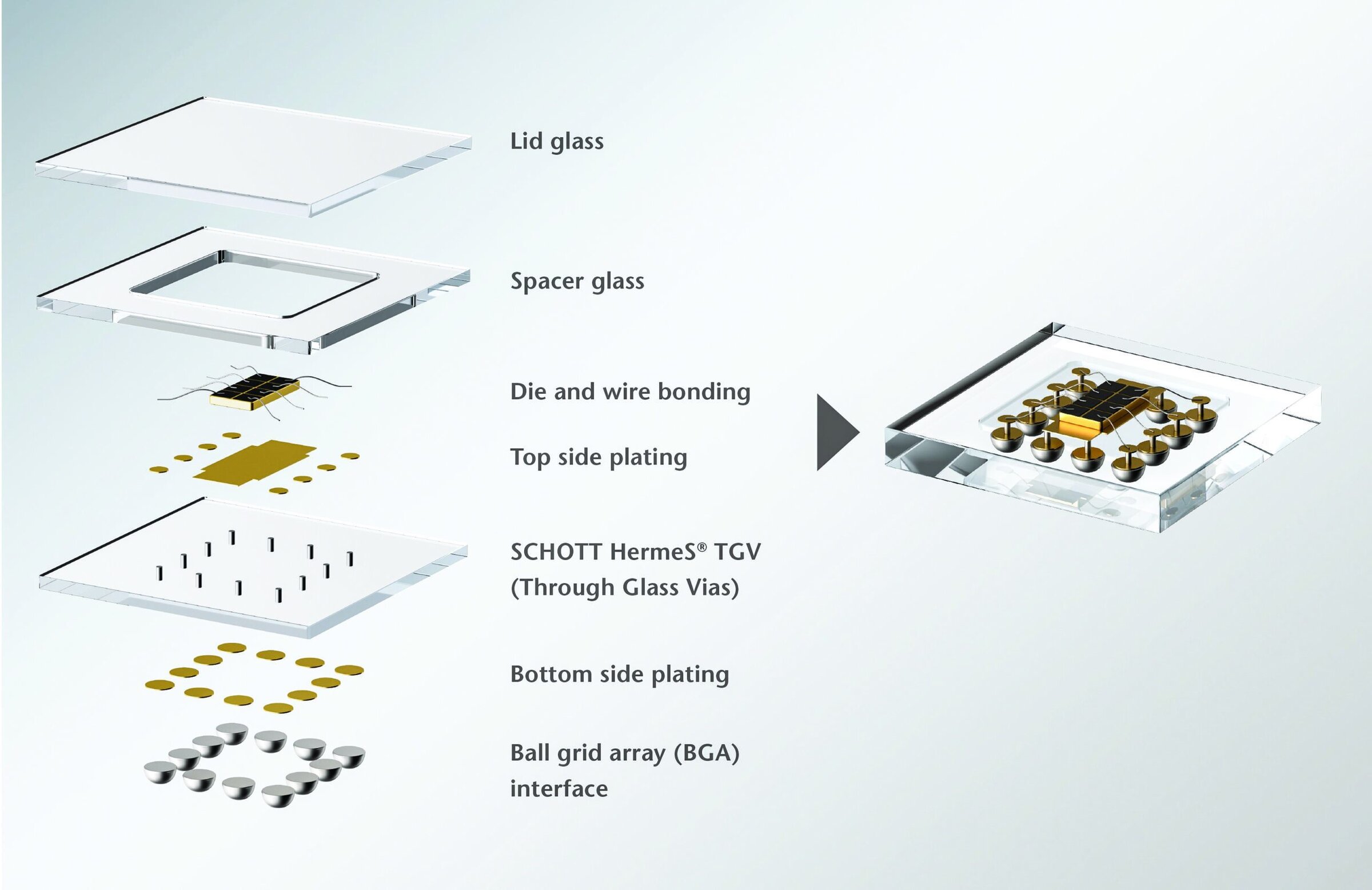
Figure 2. Schott Primoceler developed an innovative, extremely precise technology that enables additive-free, room-temperature hermetic glass bonding, enabling devices to be packaged entirely in glass. Credit: Schott Primoceler Oy
The possibilities of such technology are wide-reaching even within implantable device applications, but one of the first to see clinical application is in the eye.
For patients with reduced or lost sight due to retinal degradation, a company called NanoRetina (Herzliya, Israel) pioneered an artificial retina device. NanoRetina’s NR600 implant, which is designed to mimic the functionality of the eye’s highly sensitive photoreceptor cells, is a tiny chip containing an imager, 3D neural interface, and embedded photovoltaics to provide power. The device is completely encased in glass using Schott Primoceler technology (Figure 3).
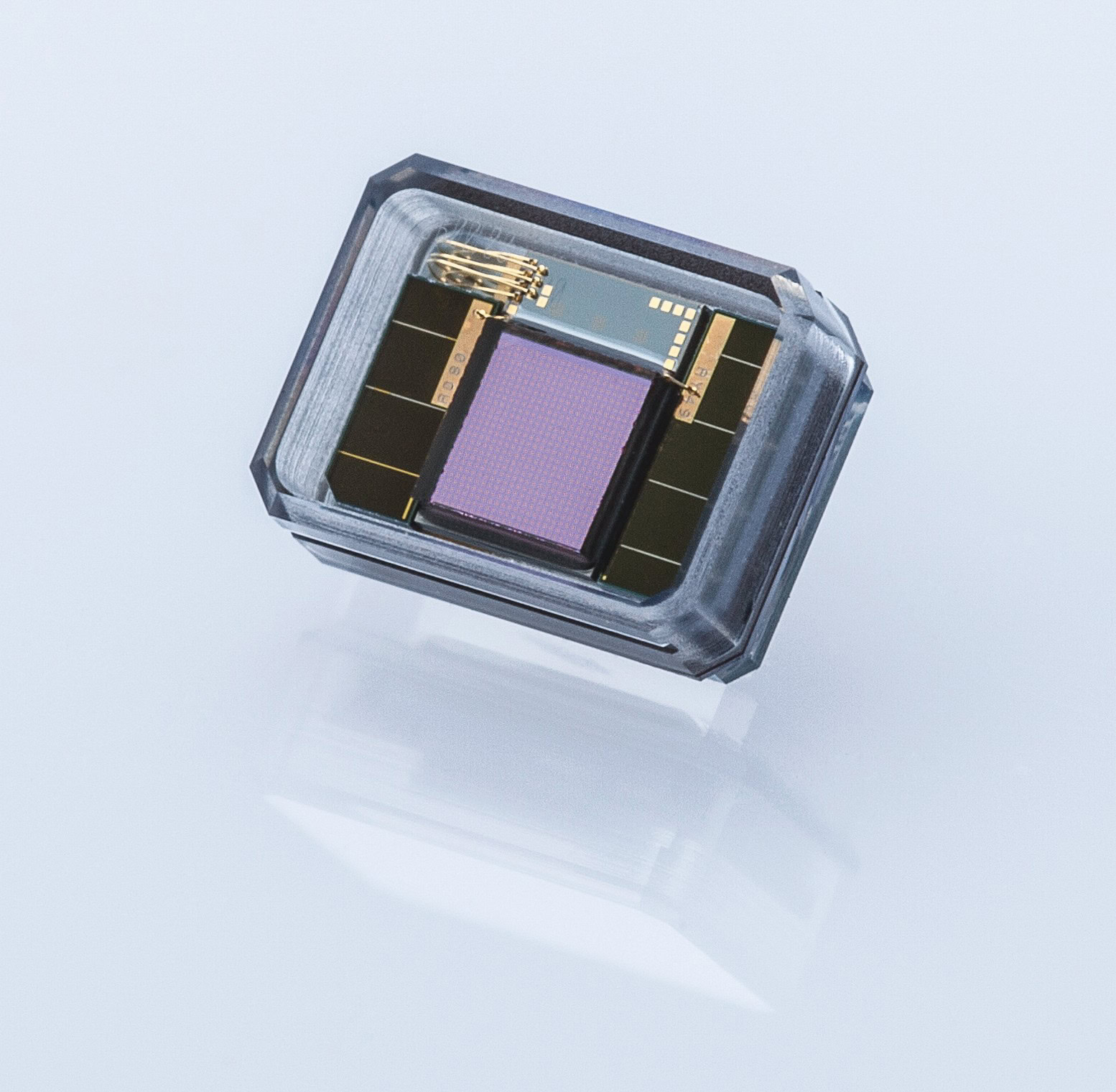
Figure 3. NanoRetina NR600 retinal implant with glass encapsulation. Credit: Schott
“Without our glass-to-glass laser bonding technology, this would not have been possible because the encapsulated sensor inside is very heat sensitive. Only with our technology could we encapsulate it at room temperature,” Herzberg says.
Enabled by glass, NanoRetina’s NR600 implant entered a small clinical trial of 20 patients in Europe and Israel in early 2020 and already shows promising results. “The device was activated for the first time, and the result was amazing: this patient had been completely in the dark for five years, and she immediately reported seeing an image in the center of her visual field when the device was activated, and could show with her hands the size of the image that she saw,” professor Peter Stalmans, who implanted the trial device and is one of Europe’s leading retinal specialists, says in a Schott press release.5 “I am very impressed by this experience. I have been working for more than 20 years as an ophthalmologist, but this is the first time I witnessed a completely blind patient being given back a visual perception.”
Akin to maturation in the smartphone industry6—where shrinking of components has enabled enhanced functionality in smaller devices—miniaturization is an important reason why implantable devices such as NanoRetina’s NR600 are possible today, and it can be traced back to advances in ceramics and glass, as well as other materials.
The consequences of miniaturization are not limited to better performing and more innovative devices, however—it also affects the ultimate bottom line in modern heathcare: cost.
“It starts with the surgery itself,” Herzberg says. “Imagine the pacemaker— 30 years ago it was very bulky, so hospitalization time of patients was really long, increasing healthcare costs. People cannot go to work, they are on sick leave, and this is very costly for insurance companies. Today pacemakers are getting smaller and smaller because technology is getting better and better.” Smaller devices allow more minimally invasive procedures, translating to faster recovery times and shorter hospital stays, which ultimately help reduce care-related costs.
Technologies and advances that continue to allow implantable devices to assume smaller forms with enhanced performance, as well as parallel medical developments that permit minimally invasive procedures and improved surgical outcomes, are critical components of future healthcare strategies to sustainably and effectively promote the health of growing, aging populations.
Joint implants: Ceramics extend implant life
Our joints, the connections between the skeleton’s more than 200 bones, provide our bodies with an incredible capacity for movement.
This ability is perhaps most appreciated in the face of reduced or lost mobility in the joints, often due to stiffening caused by conditions such as arthritis. Osteoarthritis, the most common form of arthritis, represents the single most common cause of disability in aging bodies, affecting an estimated 10%–15% of adults over 60 years old.7
As such, it is no surprise that the global market for joint replacement, implants, and regenerative product devices is expected to grow—reaching a value of $33.6 billion by 2023, growing at a CAGR of 4.8% during 2018–2023.8
Knee replacements constituted the largest share of the $26.5 billion joint replacement market (by value, not number) in 2018, accounting for 33% of the market, or $8.8 billion. Hip replacements were the next largest share, accounting for 28% of the market or $7.4 billion, followed by spinal implants (20%; $5.2 billion) and then extremities reconstruction, which comprises implant devices for the shoulder, elbow, wrist, digits, and ankle joints.
At all of these locations, ceramic implants compete with those made of polymers, metals, and combinations thereof. Due to length of time in the market, ceramics’ successful infiltration into joint replacements is most notable for hip replacements.
“Though implantable ceramics have been in the market for decades, the adoption of these materials has really happened in the last 15 years,” says Lucian Strong, vice president of CoorsTek Bioceramics (Grand Junction, Colo.), which manufactures ceramic femoral heads and acetabular liners for total hip arthroplasty, among other bioimplantable ceramic components. “The adoption is coming from the transition away from metals to ceramics due to the superior wear properties of ceramics, as well as patients’ demands for longer and more active lifestyles after joint replacement.”
Wear of polymer and metal joint implants can generate debris particles that cause inflammation around the joint, loosening the implant and potentially leading to its failure. Potential allergic reactions to metals as well as toxicity from release of metal ions from an implant into the body are also considerations.
These considerations are creating a favorable landscape for ceramic implants, and that shift is evident in data from the 2019 annual report of the American Joint Replacement Registry, a database of more than 1.5 million knee and hip arthroplasty procedures performed in the U.S. during 2012–2018. Registry data show that for total hip arthroplasty, the number of implants with ceramic heads is increasing and first surpassed those with cobalt chromium heads in 2015.9
This data, however, presents only a limited picture, as the registry captures an estimated 25%–30% of the volume of annual procedures in the U.S. Other estimates indicate that adoption of ceramic hip implants is already much higher in some parts of the world—more than 50% of hip implants performed in European countries like Austria, France, Germany, Italy, and Switzerland use a ceramic ball head, while 72% of total hip replacements in Asian countries such as South Korea have an alumina ball head.10
A large proportion of total hip replacement ceramic implants are historically alumina, although zirconia is used as well. Acceptance of zirconia was severely hindered by the 2001 recall of millions of Prozyr brand zirconia ball heads, prompted by high fracture rates in patient implants. Subsequent failure investigation of the manufacturer, Saint Gobain Ceramiques Desmarquest, determined that a switch in the type of furnace used to manufacture the implants caused an unanticipated change in temperature kinetics, resulting in insufficiently densified zirconia.11 Although the problem was traced back to a manufacturing error, the recall significantly marred zirconia’s reputation in the market.
Many modern ceramic hip joint implants now combine the best of both worlds with composites that offer improved properties of strength, toughness, and scratch resistance, for example, ones based on zirconia toughened alumina (Figure 4).

Figure 4. Femoral head and acetabular liner cup for total hip arthroplasty, manufactured by CoorsTek Bioceramics. The implant is made of CeraSurf-p, an alumina zirconia matrix composite that incorporates advanced toughening mechanisms to improve the material’s performance. Credit: CoorsTek Bioceramics
Beyond material-based considerations, additional factors also are coalescing to create a favorable landscape for ceramics implants. “Medical care has seen many transitions over time, but the latest big trend is the move to outpatient care due to rising costs,” Strong says.
Similar to how miniaturization of components allowed pacemakers to shrink in size, resulting in shorter hospital stays and lower care-related costs, parallel evolutions also occurred for joint replacements.
“Generally speaking, technical ceramics are a component of a larger medical implant. Modern ceramics are engineered to be so strong that they are allowing for design changes to the entire device,” Strong explains. “They have been optimized to the point where they are impacting the surgical procedures, which are now quicker and more efficient. In total hip arthroplasty, ceramics are a critical part of the overall device, which has been designed around the next generation in surgery. With the current trend toward robotics, these designs allow for faster and more accurate outpatient surgical procedures that previously would require significant time in hospital recovery.”
These advancements not only improve patient outcomes but also help reduce healthcare costs, factors that are intimately intertwined.
Spinal implants: Securing with Glass or silicon nitride
Because the spine provides a critical balance of flexibility and stability to the body, any modifications to the spine ideally also must balance those same properties.
Spinal implant devices stabilize and strengthen the spine in various ways, often by securing vertebral elements and inserting implants to shore up the intervertebral space (Figure 5). But that need for flexibility and stability makes spinal devices challenging to design.

Figure 5. Due to excellent their wear rates, ceramics can also be found in cervical disc bearing surfaces for spinal total disc replacements. This one, by CoorsTek Bioceramics, is made of alumina zirconia matrix. Credit: Coorstek Bioceramics
For instance, the articulation surface for a total disc arthroplasty must not only be functional, it must be designed to account for an estimated device life of more than 40 years. Considering the estimated number and amplitude of load cycles a lumbar disc undergoes annually—based on an average adult bending an estimated 125,000 times and taking 2 million steps in that year—a disc implant is expected to endure some
85 million cycles of loading during its lifetime without wearing down.12
So these devices demand incredibly high-performance and long-lasting materials. While the usual biomedical materials have long been used in spinal implant devices—metals such as stainless steel, titanium, and cobalt-based alloys offer strength; high-performance polymers such as polyetheretherketone (PEEK) provide good value—these materials do not offer perfect solutions in the spine, where integration with existing tissue is particularly desirable for preserving functionality of the spine and maintaining longevity of the device.
“Overall, the need of the hour is to develop materials that demonstrate both biomechanical applicability and biocompatibility while being user friendly in a surgical environment,” according to a 2017 article on trends in spinal surgery materials.13 So it is not surprising that this field is also starting to realize the potential of ceramics and glass.
For instance, Mo-Sci (Rolla, Mo.) is developing multicomponent bioresorbable spinal bone grafts from bioactive glass—containing one bioactive glass formulation that dissolves more quickly and contains compounds to stimulate vasculature growth (e.g., copper and zinc elements) in early stages of healing, and another bioactive glass formulation that forms a porous silicate glass scaffold that dissolves more slowly to provide support while natural bone formation gradually replaces the graft.
“This bone graft has shown really nice improvements in spinal fusion rates, and it actually isn’t even on the market yet,” says Steve Jung, chief technology officer of Mo-Sci. “Mixing to get this benefit from this material and this benefit from this material is sometimes a better option than trying to find this one material that could do it all. Sometimes you have to accept that there are just two really great materials you can put together and get what you want from each.”
Beyond bioactive glass, other materials also have their sights set on the spinal market. Silicon nitride spinal fusion devices manufactured by SINTX (Salt Lake City, Utah)—the only FDA-registered and ISO-certified silicon nitride medical device manufacturer in the world—and sold through CTL Amedica are working their way into this market (Figure 6). Silicon nitride is not only bioactive, antiviral, and antibacterial but also promotes bone growth, providing an effective orthopedic solution.

Figure 6. Silicon nitride spinal devices manufactured by SINTX. Credit: SINTX
Although the material currently constitutes a small portion of the overall market for spinal fusion devices, data indicates silicon nitride has significant potential, as the company reports there were fewer than 30 FDA-reported adverse events despite more than 35,000 human spine implantations over 10 years.10
SINTX anticipates many additional orthopedic applications for silicon nitride, such as dental and craniofacial applications as well as joint replacements. “There’s a lot of concerns that metals corrode in the body. As you’re putting hips into younger and younger patients who are going to live longer, you’re not looking at 20-year outcomes. You’re interested in 30- and 40-year outcomes, and there ceramics have a very special role,” says Sonny Bal, president and CEO of SINTX.
For craniofacial applications, customized repair of defects with 3D-printed patient-specific implants is a possibility that SINTX has in mind, according to Don Bray, vice president of business development at SINTX. “If someone has a severe accident and you need to rebuild the facial bones and structure, you would want to do a CAT scan and make an exact fit. In the spine you can use some standard sizes. But because of the shape of the face, you can’t—and we think 3D printing there with our silicon nitride is key,” Bray says.
“It’s a very critical area, so having an antibacterial implant that would you could make exactly for the person is where we think this is going to go,” Bray adds. “And we don’t think it’s that far off.”
Because of silicon nitride’s favorable antibacterial and biological properties, SINTX also is developing techniques to incorporate silicon nitride into devices and products made of other materials as well. For example, silicon nitride can be mixed into polymer-based products or coated onto titanium devices to enhance biocompatibility of those surfaces, promote healing, and prevent infection and spread of viral diseases, according to Bal. “We are looking at 3D processing procedures that we can commercialize, in which we put a very tenacious micron-level coating of silicon nitride that supercharges the metal and makes it antibacterial,” he says.
3D printing: A technology with layered medical potential
Multimaterial implants
At the intersection of medical care and additive manufacturing lies tremendous promise to completely change how we approach health strategies to replace, enhance, and restore function of the human body.
According to the annual Wohler’s report, the 2019 additive manufacturing industry was worth some $11.867 billion. Medical and dental applications account for about 11% of that market, and dental in particular represents a large growth segment in the latest report.14
Additive manufacturing company Lithoz GmbH (Vienna, Austria) is familiar with the potential of the technology for medical and dental applications. Lithoz’s lithography-based ceramic manufacturing technology 3D prints complex structures layer-by-layer using a photocurable polymer–ceramic slurry. After printing, green parts are debinded and sintered to remove the polymer, leaving fully dense ceramic parts.
Lithoz developed both the expertise and the custom printers to additively manufacture a diverse array of ceramic materials, everything from piezoceramics to regolith, and certainly including ceramics with medical applications such as alumina, zirconia, silicon nitride, hydroxyapatite, and tricalcium phosphate. Daniel Bomze, head of the Lithoz’s medical business unit, says the company also has success printing with bioactive glass. “We have produced several parts and some slurries already successfully with bioglass. So we know it works,” he says. Now, Bomze says Lithoz is waiting for a commercial partner who is interested in making the investment to further develop applications for additively manufactured bioactive glass.
Lithoz’s technologies can print complex geometries such as high-resolution lattice structures with openings just several hundred microns wide—optimal scaffolds to promote interaction and integration with living tissues—so medical applications are one promising direction (Figure 7). For instance, such bioceramic scaffolds could be used to repair bone defects due to injury or disease.
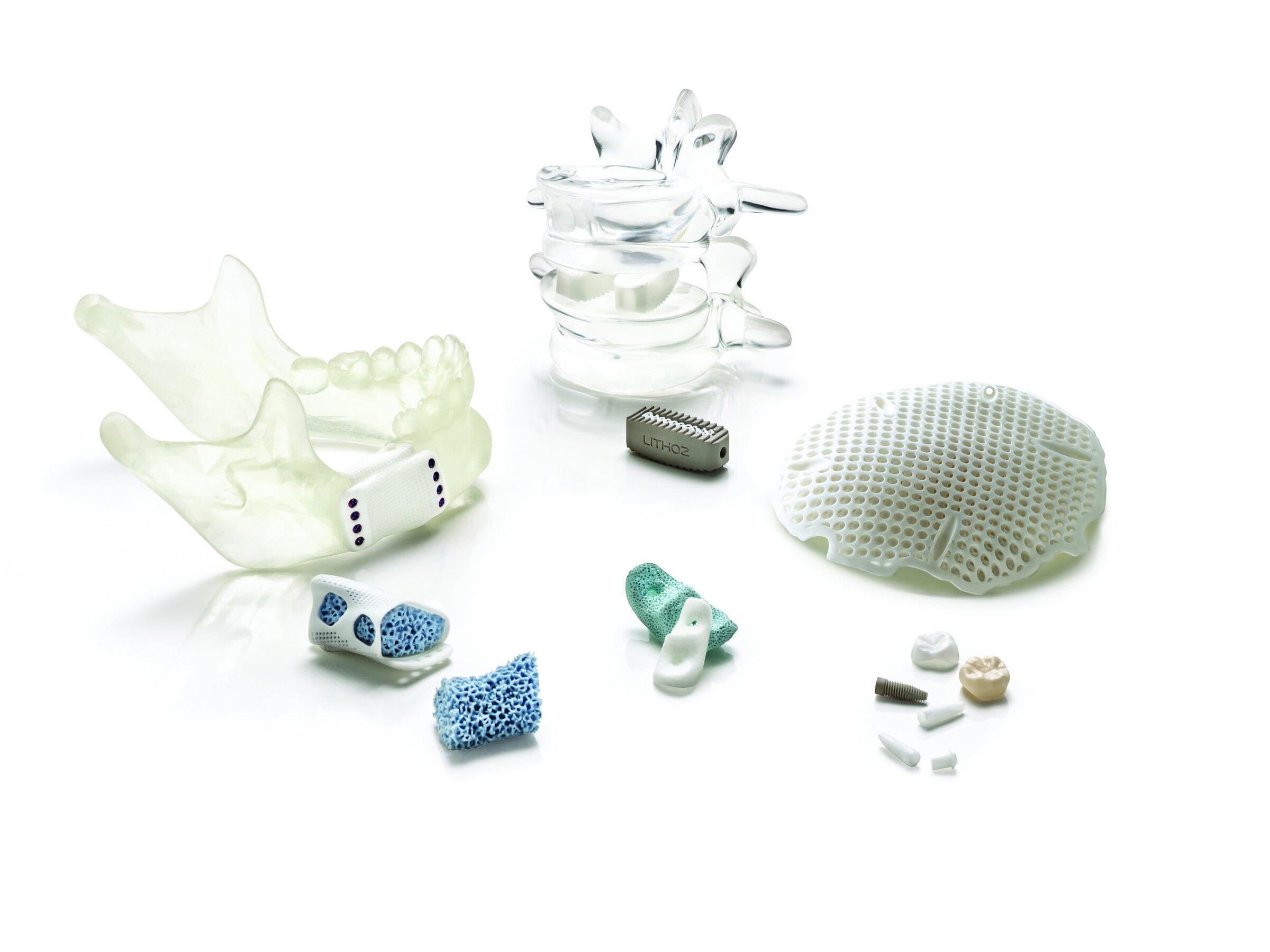
Figure 7. 3D-printed medical devices manufactured with Lithoz CeraFab System printers. From left to right: a) Mandibular implant (white: zirconia, blue: hydroxyapatite), b) spinal implants (grey: silicon nitride, white: tricalcium phosphate), c) front jaw bone augmentation (blue: hydroxyapatite, white: bioactive glass), d) cranial implant (tricalcium phosphate), e) zirconia crowns (native and colored), f) dental implants and abutment (grey: silicon nitride, white: zirconia). Credit: Lithoz
While ceramic and bone are a perfect match materially speaking, design of bioceramic scaffold structures is challenging because they must provide both porosity and mechanical strength, properties that often come at a tradeoff. Fortunately, natural bone can provide some inspiration. Bone’s structure consists of an outer layer of dense cortical bone filled with porous and spongy inner trabecular bone, a multimaterial strategy that uses two different forms to provide two different components of bone’s function.
Lithoz is developing multimaterial 3D-printed implants that provide both porosity to promote tissue regeneration and mechanical stability to support a bone defect. These multimaterial implants incorporate a strong outer layer for structural support during the initial healing phase, composed of a ceramic material with good mechanical stability such as zirconia, with a porous inner scaffold of bioresorbable ceramic substrate such as tricalcium phosphate or hydroxyapatite. The inner material more closely matches the inorganic component of bone, and its porosity permits cell attachment and penetration of blood vessels, allowing the body to heal and replace the bioresorbable substrate with natural tissues over time.
Such multimaterial implants could be used to repair many types of bone defects, such as those in the jawbone. Critically, Bomze says, the material’s resorption rate can be tuned to the area of the body being targeted. “The ideal would be that the regrowth, the new tissue forms at the same speed as the implant is being resorbed. So you have the overall volume and stability, and the whole healing time is the same by tuning this artificial material and the natural material,” he says.
Although the individual components of these implants were implanted into a small number of human patients, with good results so far, the multimaterial implant is currently a proof-of-concept. And although the current design is printed into two separate steps, Lithoz has bigger plans for the future.
“The future will be printing it simultaneously, in one single step—you could print the cage and the inner part at the same time and then sinter them together,” Bomze says. “You can probably make even more sophisticated materials, for example a sandwich structure with an inner part of hydroxyapatite, then a shell of zirconia, and then a tiny outer coating or a third layer again of hydroxyapatite to facilitate ingrowth of the of implant. And here we’re making really rapid progress.”
In that vein, Lithoz released in September 2020 a new multimaterials 3D printer called the CeraFab Multi 2M30. The printer is similar to the company’s other offerings but now includes two vats to provide the ability to simultaneously print with two different raw materials (Figure 8). This ability affords new functional applications, such as printing multiple materials in a single layer and allowing gradual compositional variation from one material to the next.15
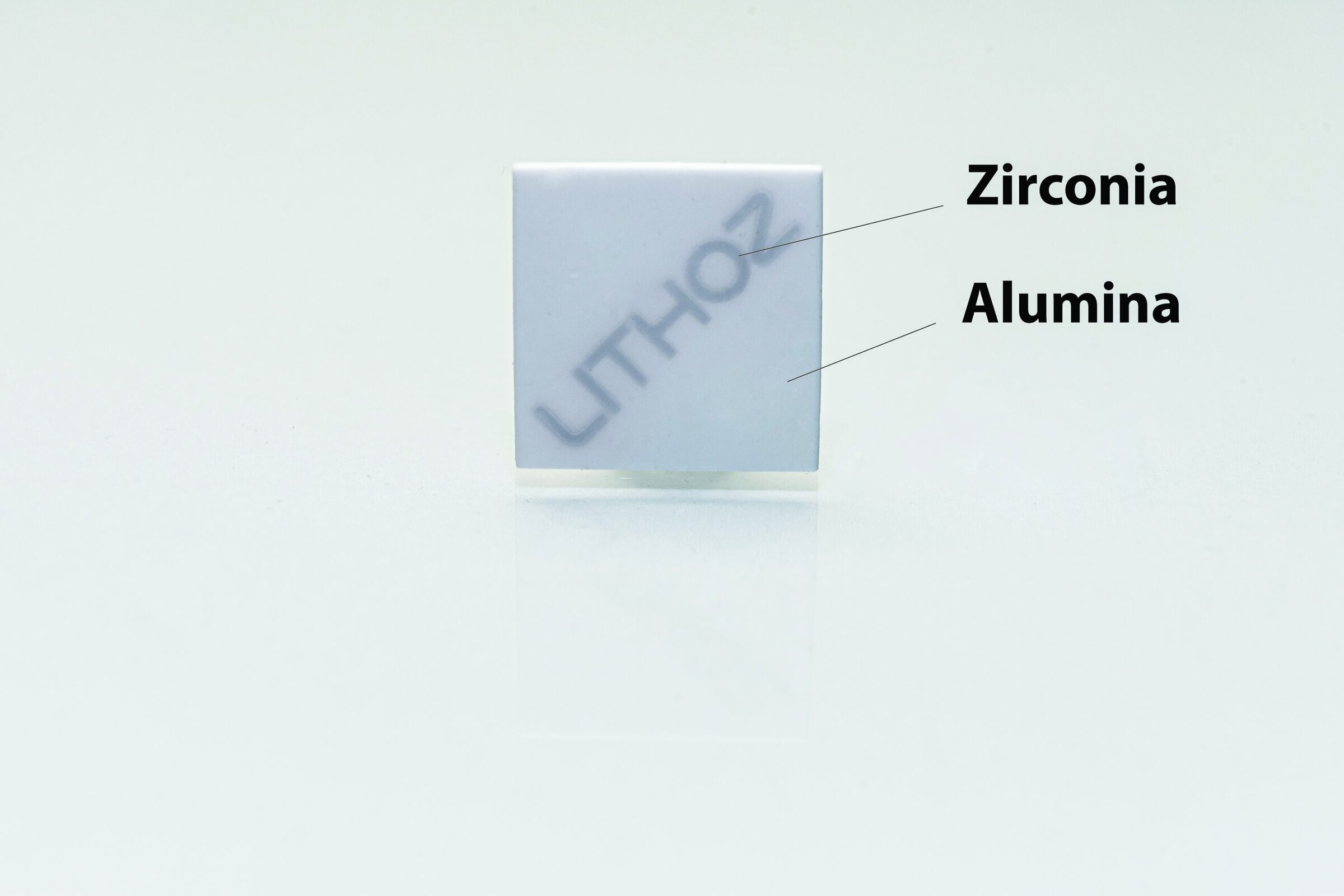
Figure 8. A multicomponent demo part made of alumina (outside) and zirconia (inside, Lithoz writing) printed on a CeraFab Multi 2M30. Both materials were printed in one run simultaneously, and the part is sintered. Credit: Lithoz
3D-painting
Additive manufacturing is a diverse technology, so Lithoz’s lithography-based technique is one of many different approaches.
Another company, Dimension Inx (Chicago, Ill.), is innovating with printing ceramic-based biomaterials at room temperature, with no additional post-processing sintering steps required—affording the ability to incorporate organic molecules such as proteins, drugs, and antibiotics into the materials themselves before printing.
As noted in a May 2019 Bulletin article,16 “3D-painting is a materials-centric advanced manufacturing technology that permits nearly any material to be transformed into a 3D-printable ‘3D-paint’ via simple, room-temperature extrusion without the need for support materials, powder-beds, resin-baths, cross-linking, or curing.”
In the 3D-painting technique, a powder-based material is mixed with elastomer and solvents; after extrusion through a nozzle, the finished printed product requires only rinsing and sterilizing. The flexibility of the technique means that in addition to 3D printing structures out of 3D-paints, the same strategy could also be used to coat products manufactured via other techniques and out of other materials.
Importantly, 3D-painting can be applied to almost any material, including ceramics. “3D-painting is materials agnostic. It’s not dependent on what you’re making or what material you’re using,” says Adam Jakus, co-founder and chief technology officer at Dimension Inx.

Figure 9. Anatomical structures display a handful of possible structures that were 3D printed by Dimension Inx with Hyperelastic Bone: (clockwise, from top left) spine, femoral head, mandible, and pelvis. Credit: Adam Jakus, Dimension Inx
As one example of the 3D-painting technology, Dimension Inx’s bone-specific 3D-paint formulation, called Hyperelastic Bone®, is primarily ceramic yet still incredibly flexible, offering significant potential for bone implants. Hyperelastic Bone can be printed in specific structures (Figure 9) as well as porous scaffolds and sheets that could be cut and custom-fit in the operating room (Figure 10).

Figure 10. A sheet of Dimension Inx’s 3D-printed Hyperelastic Bone, which is flexible despite being 90% ceramic. Credit: Adam Jakus, Dimension Inx
“The really interesting thing about Hyperelastic Bone is that it’s 90% ceramic, which is technically more ceramic than is in our actual bones,” Jakus explains. Human bones contain 60%–70% dry weight of crystalline hydroxyapatite, bound by collagen and other structural and functional proteins. “But the end result is actually flexible and cuttable and shapeable, which you wouldn’t really expect for a something that’s mostly ceramic.”
That flexibility is because of Hyperelastic Bone’s unique microstructure, which forms as evaporants vaporize from the printed material after it is extruded through a printer nozzle. The rate of evaporation tunes precipitation of the elastomer, forming an optimized structure in the printed material.17
“A very specific microstructure really allows the different components of the composite, the ceramic and the resorbable polymer, to play off each other and move around and then return to their original form without breaking,” Jakus says.
Hyperelastic Bone also is microporous, which provides excellent osteoconductivity and biocompatibility. “If it’s intended to regrow bone, the body tissue needs to be able to access that material on the microstructure level and transform it,” Jakus says, although the porosity can have a drawback. “But it’s a balance if you want structural integrity and you want bioactivity. Those things are in conflict all the time.”
Since the technology is relatively well-established at this point, Jakus says Dimension Inx is now working on quality control aspects of the process, showing that it can demonstrate consistent results. “So a lot of our efforts throughout 2020 have been establishing new quality control systems and quality manufacturing systems around design and synthesis of these new materials as well as the 3D-painting process itself,” he says.
That includes establishing consistent and detailed manufacturing processes and identifying and mitigating risks—all part of the company’s preparations toward seeking FDA approval for Hyperelastic Bone devices.
3D printing inherently conjures ideas of patient-specific printed implants. And while that is an eventual direction for Dimension Inx, the company is starting with a more practical pathway—and one common for biomedical innovations—by targeting mass-produced implants of Hyperelastic Bone, a collection of standard shapes like “strips or squares or blocks,” Jakus says. “We are introducing a new material in a new manufacturing process. So I think it’s important to get the regulatory agencies, the FDA, surgeons, everybody comfortable with the material and the process first so they are then willing to take that next step to patient-matched implants.”
That acceptance is a considerable issue in the medical industry—you not only have to prove that a device or technology works (see sidebar: Regulating the pace of medical innovation), but you also have to convince medical professionals to use it as well. And that can be a major barrier, especially for new medical innovations.
“The technology is the easy part,” Jakus says. “And even after you identify a technology that addresses an actual need, getting surgeons to venture out their comfort zone is very hard.” If an existing clinical solution is trusted and works relatively well, medical professionals often are not keen to change a process, especially if the solution does not offer additional profit or patient benefit or it requires the professional to master a new technique. Introducing a new product also comes with some inherent risk, which medical care is designed to minimize, for good reason.
One sector, however, where medical professionals are often more willing to take modest risks is the craniofacial space—which is why medical innovations often target this site.
In particular, additively manufactured medical technologies often focus on craniofacial applications because these defects are non-load bearing and highly individualized. In addition, there are few existing off-the-shelf products to treat craniofacial defects, so these medical professionals are often more willing to take a slight risk with innovative new solutions.
Infiltrating a site like the craniofacial space can then be a strategic initial target application of a new technology to gain acceptance before expanding to additional sites and applications.
Another consideration that makes the craniofacial segment attractive for innovation in additive manufacturing, especially with bioresorbable materials, is that these surgeons treat many pediatric defects. “So they’re most excited to use new materials, ceramic or not, that transform over time and grow with the patient,” Jakus says.
Tissue regeneration: The softer side of biomaterials
In terms of the body’s natural materials, ceramics and glass are most analogous to bone and tooth enamel—so it is not surprising that there are so many orthopedic and dental applications for ceramics and glass (see sidebar: Ceramics used in dentistry).
But modern developments in nanotechnology, particularly the ability to engineer nanosurfaces, nanoparticles, and nanoscaffolds, as well as more nuanced understanding of cell biology are together reshaping how we think about the potential of biomaterials.
Biomaterials were once designed to minimize interactions with the body and to eliminate any potential adverse reactions. But starting with Larry Hench’s discovery of bioactive glass 50 years ago,18 a more modern perspective for biomaterials no longer attempts to eschew cell biology.
“Design of a new biomaterial should always consider the need of the cells, because the cells are the engineers of our body,” says Aldo Boccaccini, professor of biomaterials and head of the Institute of Biomaterials in the Department of Materials Science and Engineering at University of Erlangen-Nuremberg (Erlangen, Germany).
Many biomaterials now aim to not only stand in for living tissues when they need to be repaired or replaced, but the materials play a more supportive role in actually helping the body perform its own healing—more like an assist rather than a complete substitution. That guidance can be used to mediate processes such as wound healing and to rebuild damaged or missing tissues, broadly contributing to the overall field of tissue engineering, or regenerative medicine.
In terms of the future of healthcare, regenerative medicine is a big business. The global market for tissue engineering and regeneration was valued at $24.7 billion in 2018 and is predicted to reach $109.9 billion by 2023, representing an impressive CAGR of 34.8%.19 While bone is a significant focus of this market, it encompasses soft tissues as well, such as strategies to repair damaged cardiac and gastrointestinal tissues or engineer vascular, muscle, neural, and skin tissues.
Likewise, there is potential for many different types of materials in this broad field. “In the field of regenerative medicine and tissue engineering, there is no one material that is going to tackle all the problems,” Boccaccini says. And many of the ceramic- or glass-based strategies to heal tissues actually combine them with organic materials, in polymer composites or hydrogels, for example.
Although bioactive glasses were discovered half a century ago, their potential within regenerative medicine is still being realized today. When in contact with body fluids, bioactive glasses dissolve and release ionic dissolution products such as biologically active ions within the body. Cells, in turn, respond to these ionic products, some of which stimulate growth of new blood vessels in the tissue, a process called angiogenesis. Blood vessels nourish developing tissue with oxygen and nutrients and remove waste products, so the angiogenic response is part of what makes bioactive glass so attractive for tissue repair.20
But ionic dissolution products also do more than stimulate angiogenesis—these products alter gene expression patterns in nearby cells, shifting signaling pathways that orchestrate every cellular function, such as cell migration, proliferation, and differentiation.
Although we are just beginning to unravel some of these biomolecular mechanisms, the potential exists for bioactive glass compositions and properties to catalyze a diverse array of cellular responses, precisely tuned to the target tissue and the desired effect in that tissue—whether that is modulating an immune reaction, prompting tissue regeneration, or stimulating release of growth factors to guide stem cell differentiation.
“Understanding genetic upregulation and activation by ionic stimuli released from bioactive glasses offers the possibility of developing patient-specific therapies, a huge challenge for the aging population,” per a 2015 Bulletin article on bioactive glasses.21
One of the more familiar and clinically approved applications of bioactive glasses for soft tissues is in wound repair, with products such as a cotton candy-like borate bioactive glass fiber matrix to heal advanced wounds.22
“But you can also think of internal wounds, such as adhesives with hemostatic ability for coating internal wounds where there is a lot of bleeding,” Boccaccini says. “Here I think yet is an open area for the applications of [bioactive glass], either as a fiber or mesh or in composites.”
As research continues to characterize how cells respond to the unique materials as well as the underlying biomechanisms of these responses, soft tissue applications of bioactive glass will also continue to expand.
Mo-Sci’s Steve Jung says that bioactive glass is experiencing increasing integration in medical products due to the material’s recognition as a “premium material” and its ability to intimately interact with tissues. Bioactive glasses are being combined with other materials to make new products as well as being integrated into existing products already on the market. “They’re making these products better by the addition of bioactive glass,” Jung says.
Jung says that in veterinary medicine, there also have been some indications that bioactive glass can also repair tendons and ligaments. “To me, that kind of outcome is really what gets you thinking about sports injury-type situations—if you blow a ligament, could we develop a technology to help to heal that back together?” he says.
Beyond being implanted within the human body to aid tissue regeneration, ceramic and glass materials can also be similarly used to grow tissues outside of the body, with the vision that these tissues could eventually be harvested and implanted into or on the body as appropriate.
“The possibilities for ceramic technologies for improving the health and wellbeing of mankind are vast,” says Randel Mercer, chief technology officer at CoorsTek. “One exciting avenue CoorsTek has been working on is the use of engineered ceramic cell culturing devices. Our product, Cerahive, is used to grow human tissue cells in an environment that mimics the growth environment in the human body.” These porous ceramic substrates line the bottom of a cell culture dish to support 3D cell cultivation, allowing in vitro growth of cell spheres (Figure 11). “The future potential to ‘manufacture’ specific tissues in the laboratory could be used as a source for repairing damaged tissue in humans,” Mercer says.
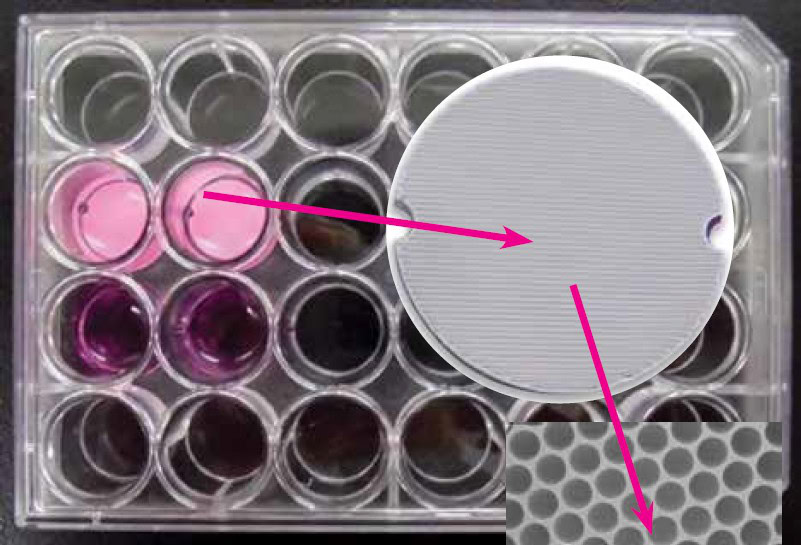
Figure 11. CoorsTek’s Cerahive 3D cell cultivation system. Small porous ceramic discs placed in the bottom of a cell culture disc allows growth of 3D cell spheres in vitro. Credit: CoorsTek
Looking forward—a glimpse of future healthcare
So what does the future of medical care look like, and how do biomaterials fit into that future?
“The medical industry is constantly searching for new, better, and more cost-effective solutions, and advancements in the medical industry are moving at a pace so much faster than just a few years ago due to the introduction of advanced materials. With climbing healthcare costs combined with the move from inpatient to outpatient procedures, there is a pull from the market for better materials,” says CoorsTek’s Lucian Strong.
Ceramics and glass clearly fit into that future vision not only because of the role of established products such as joint implants but also due to entirely new forms and functionalities of the materials that are just starting to be discovered, realized, and matured.
“I absolutely believe that ceramics and bioactive glass have a really strong future, and their areas of use are going to diversify in a big way,” says Mo-Sci’s Steve Jung. “Bioactive glass is 50 years old, but we’re still finding new ways to use it all the time. Old materials used in new ways or in combination with new techniques I think is the wave of the future.”
Some of those new ways, combinations, and techniques are highlighted in this article, but potential extends much, much further as well.
One particular area ripe for future innovation is technologies that address multiple different tissues simultaneously. Although an isolated tissue-specific approach often guides biomaterial developments, components of the human body operate together in systems on several different scales.
“If you look at everything in isolation, there are solutions that already exist. They may not be the best solutions, but there are ways to treat individual tissues,” says Dimension Inx’s Adam Jakus. However, most injuries or conditions involve multiple tissues, so more complex solutions are often required.
“This has been a driving force for our technology for a long time, and we set up a manufacturing technology where all the materials are complementary to each other,” Jakus says about Dimension Inx’s 3D-painting platform. “So we can manufacture a bone material with a muscle material and with a ligament material, so that in the future you could make a multitissue implant.”
Such strategies will inevitably need to leverage properties and strengths from multiple different materials. “This could be partially ceramic, partially polymer, partially biological, even partially things like graphene and graphite for electrical conductivity,” Jakus adds. “So manufacturing different material types together to match the really different material types in the body.”
Another systems-level approach that will certainly shape the future of healthcare is smart implants.
Miniaturization of devices, enabled by advances in the materials themselves, provided the feasibility for tiny sensors that can be implanted within the body to track an array of biological parameters on-demand. Such sensors provide the ability to track those parameters continuously, rather than sporadic measures taken at a doctor’s office or hospital, and monitor for any changes that could signal a potential health problem. Such rich data provides a more comprehensive view of a patient’s health as well as the ability to respond immediately to a potential disturbance in that health.
According to Schott’s Jochen Herzberg, smart implants have a prominent place in the future of medical care not only because they provide better monitoring but also in terms of reducing healthcare spending, by reducing trips to the doctor or hospital and by informing more strategic medical intervention when necessary.
“A trend that is very visible right now is smart implants and remote monitoring of patients to reduce hospitalization. For example, in-line measurements of vital signs like blood pressure inside of your body, with smart computers inside your body communicating with your doctor without being hospitalized,” Herzberg says.
Glass is already used in several different components of such devices, including hermetic seals, but its optical transmissivity offers compatibility in terms of data transmission (see sidebar: Could future bandages not only be smart, but also made of glass?).
Yet tiny implantable devices also can do more than just sense and monitor—they can also be designed with the capability to intervene as well, for instance by delivering a therapeutic.
“This is very fast moving technology. The idea is to replace conventional medical therapies with active implants so that you avoid overmedicating your whole body, for example by replacing implants that are active only where the pain is created rather than influencing the whole body,” Herzberg says.
Smart implants play into an overall health ecosystem increasingly focused on early detection and proactive intervention, before health conditions because problems and require more involved treatment.
These data-based monitoring strategies extend beyond implants as well, according to a Deloitte Insights report on the future of health.23 “Medical products might no longer be limited to pharmaceuticals and medical devices. They could also include software, applications, wellness products, even health-focused foods. The home bathroom of the future, for example, might include a smart toilet that uses always-on sensors to test for nitrites, glucose, protein, and pH to detect infections, disease, even pregnancy. A smart mirror equipped with facial recognition might be able to distinguish a mole from melanoma,” the report says.
Ultimately, the entire landscape of how we approach, monitor, manage, and mitigate human health is shifting. While these changes will not come without challenges to the market for biomaterials, they also offer incredible opportunity—and ceramics and glass are certainly well-positioned to capitalize on such opportunities as well as integrate critical function into the human body.
Acknowledgements
We thank Carolyn Primus for her review of and detailed suggestions for the section “Ceramics used in dentistry.”
Read more: “The science and art of glass ocular prostheses“
Read more: “Breathalyzers: Another way to detect COVID-19“
Read more: “Regulating the pace of medical innovation“
Read more: “Ceramics used in dentistry“
Read more: “Could future bandages not only be smart, but also made of glass?“

Related Articles

Market Insights
Engineered ceramics support the past, present, and future of aerospace ambitions
Engineered ceramics play key roles in aerospace applications, from structural components to protective coatings that can withstand the high-temperature, reactive environments. Perhaps the earliest success of ceramics in aerospace applications was the use of yttria-stabilized zirconia (YSZ) as thermal barrier coatings (TBCs) on nickel-based superalloys for turbine engine applications. These…

Market Insights
Aerospace ceramics: Global markets to 2029
The global market for aerospace ceramics was valued at $5.3 billion in 2023 and is expected to grow at a compound annual growth rate (CAGR) of 8.0% to reach $8.2 billion by the end of 2029. According to the International Energy Agency, the aviation industry was responsible for 2.5% of…

Market Insights
Innovations in access and technology secure clean water around the world
Food, water, and shelter—the basic necessities of life—are scarce for millions of people around the world. Yet even when these resources are technically obtainable, they may not be available in a format that supports healthy living. Approximately 115 million people worldwide depend on untreated surface water for their daily needs,…