
Ages of human history and progress have been defined and titled by our ability to access, manipulate, and master use of certain materials—stone, bronze, iron, steel, and silicon—to create new technologies and shape the world. However, throughout the course of this history, the human condition and form have arguably changed very little. Humans today are still comprised of the same complex materials as the ancestors of thousands of years ago.
This bodily materials harmony is frequently disrupted by injury or illness—just like damaging a material—which has prioritized medicine among many societies. Despite long, parallel histories, it has only been in the past few decades that the fields of medicine and materials science and engineering have begun to intimately converge, yielding what may be considered the beginning of the age of advanced biomaterials. At the same time, advanced manufacturing technologies, such as additive manufacturing and 3D-printing processes, are enabling clinical use of traditional and emerging advanced biomaterials.
With this three-way convergence of biomaterials, medicine, and advanced manufacturing, it is now becoming possible to access, manipulate, and master the use of biomaterials for tissue repair and regeneration. But what kind of materials can recapitulate the natural form and function of complex biological tissues, or even transform into those tissues after implantation? And how can those materials be formed to fit the human body?
A great need for bone reparative materials
Many materials comprise the human body. But at its core are more than 200 bones that provide both structural support and systemic, functional support. Bones are ceramic composites with incredible properties, but they are not immune to damage or failure. If you have not personally suffered from a bone-related injury at some point in your life, there is a good chance you know someone who has.
Despite ongoing improvements in preventative and restorative healthcare, boney defects such as those resulting from congenital abnormalities, osteotomies (bone cancer removal), and trauma can be physically debilitating, socially incapacitating, economically burdensome, and even deadly.1 Thus, there is significant need for not only technically effective bone repair and regeneration treatments, but, given the scale of the problem, solutions that also are cost-effective.
Conventional treatments to repair or replace bone include use of autologous bone grafts (bone removed from one part of the body to treat a defect in another), allografts (material from human cadavers), and/or synthetic materials. However, these strategies currently suffer from several limitations and deficiencies, including donor site morbidity and pain (autograft), inconsistency and risk of infection (allograft), and minimal tissue integration and bone repair (synthetics).
Thus, based on extensive global medical need and existing material deficiencies, more resources are being devoted to develop ceramic-based biomaterials that take advantage of natural tissue regenerative responses, a field known as tissue engineering and regenerative medicine, to effectively treat both orthopedic and craniofacial boney defects.
Tissue engineering and regenerative medicine
The field broadly referred to as tissue engineering and regenerative medicine (TERM) has been active for 30–40 years and generally seeks to leverage individual and combined properties and potential of three major systems—living cells, external stimuli (e.g., chemical, electrical, mechanical), and scaffolding materials—to create or biofabricate reparative, regenerative, and/or replacement constructs that recapitulate biological form and/or function.
From a cellular perspective, hundreds of distinct cell types comprise the human body. Cells constantly produce and utilize various bioactive molecules, such as growth factors and structural proteins, that act as instructions, building components, and stimuli. With so much dynamic complexity, it may seem futile to try to reconstruct existing or create new biological tissues and organs.
However, the same complexity that makes the task of addressing biological tissues and organs appear so challenging also has a major benefit—the body is smart and can respond to, integrate with, and reform and repurpose implanted materials and structures.2 Regardless of the approach, the resulting technology must meet numerous technical, surgical, economic, and regulatory criteria (Figure 1).
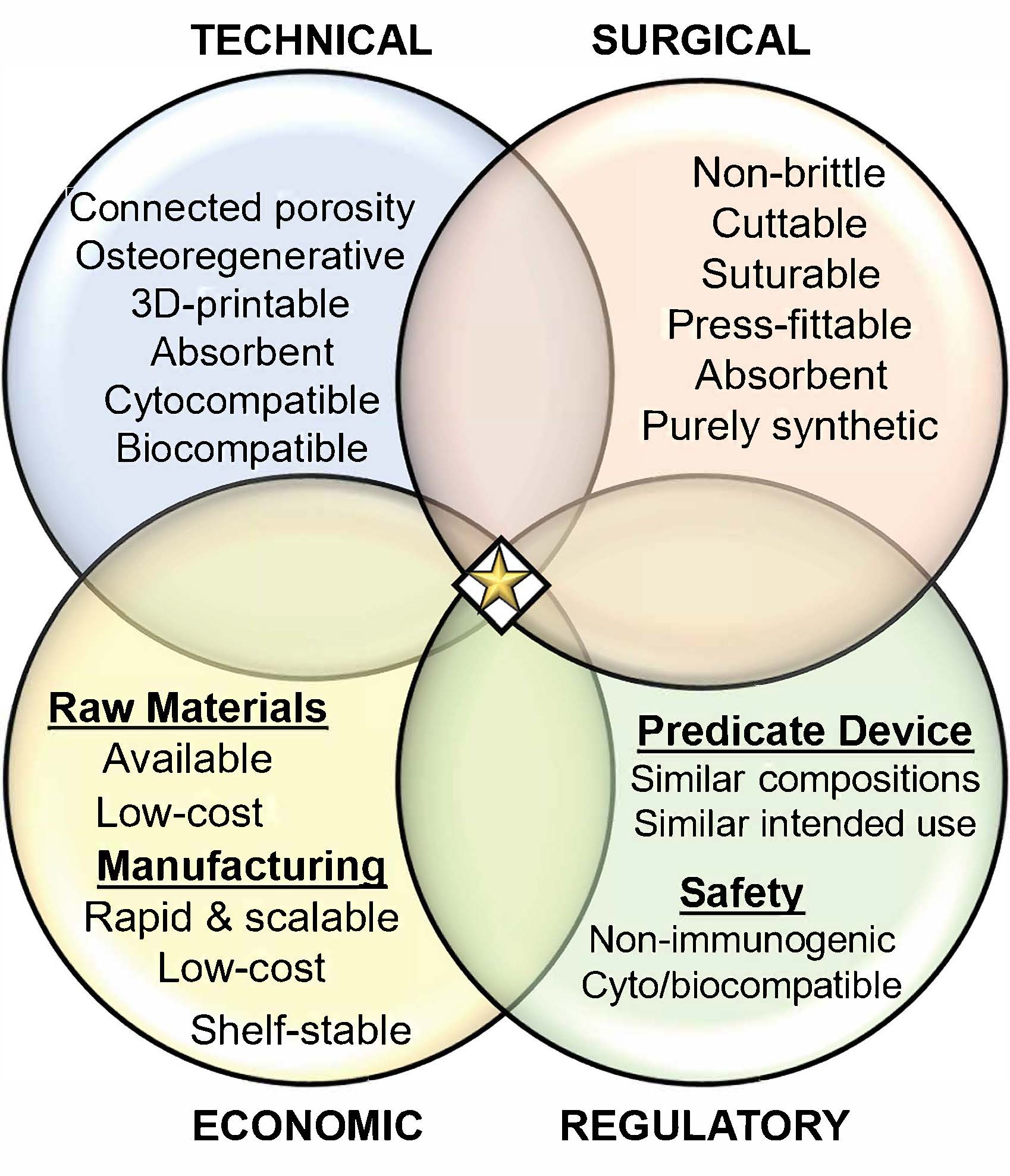
Figure 1. Technical, surgical, regulatory, and economic criteria all must be satisfied to yield an ideal ceramic-based biomaterial (star) for bone repair and regeneration. Credit: Adam Jakus, PhD – Dimension inx
A brief introduction to bone composition and structure
The foundation of TERM approaches relies on introducing material compositions and structures to the body that can be recognized by host cells, integrated with surrounding biology, and transformed to have both form and function of native tissues. Thus, it is important to understand the targeted tissue—in this case, bone.
Bone is a natural composite of discrete, ceramic particles (60–70 percent by dry weight) bound together in a porous matrix by ordered collagen protein, a natural structural polymer (25–30 percent by dry weight), and additional structural and functional proteins. The ceramic component of human bone is crystalline hydroxyapatite, Ca10(PO4)6(OH)2.
Two primary types of boney structures exist: cortical or compact bone, and trabecular or spongy (also known as cancellous) bone. The cortical structure makes up the exterior of bones and provides structural strength, while the interior trabecular structure houses bone marrow, which generates red and white blood cells as well as platelets.
The function of bones thus extends far beyond structural support. Therefore, permanent implants made of metals and polymers, which may only impart the structural function of bone, are not ideal materials for bone repair and replacement, Ceramics, which can potentially transform into new bone, are ideal materials.
Ceramic-based biomaterials for bone repair and regeneration—technical considerations
For a ceramic-based biomaterial to be effective, it must meet numerous compositional, physical, biological, and structural criteria. Compositionally, ceramic-based biomaterials intended for bone repair and regeneration should be or should exhibit resemblance to the calcium phosphate comprising natural bone, hydroxyapatite. It is for this reason that hydroxyapatites and additional calcium phosphates, such as beta tricalcium phosphate, Ca3(PO4)2, in the forms of powders, granules, putties, and cements are widely used as bone grafting materials.
Other ceramics, including calcium carbonates and sulfates as well as silicon nitrides and carbides, are also finding increasing clinical use. Additionally, ceramics doped with strontium or zinc ions, further emulating the composition of bone, have yielded improved bone repair over base ceramic efforts.3 Beyond ceramics, glasses such as bioglass4 are also increasingly used to treat boney defects. Growth factors such as synthetically derived bone morphogenic proteins (BMP), which are found naturally in bone tissue, are also frequently added to implants to increase bone formation.
Biologically, the material/structure must be safe and must not elicit a strong, negative immune response after implantation. The immune response will be mitigated if the implanted structure rapidly integrates with its surroundings. This tissue integration and its corresponding vascularization are also necessary for the implant to achieve its primary purpose of bone repair and regeneration.
The details are beyond the scope of this article, but new bone formation can be achieved via two mechanisms: osteoconduction (new bone growth from existing bone) and/or osteoinduction (new bone growth independent from existing bone). Many ceramic-based biomaterials, such as those described previously, are osteoconductive in nature but lack inherent osteoinductivity without addition of bioactive factors such as BMPs.
From a physical and structural perspective, the implanted ceramic should be highly porous and absorbent (“liquid wicking”), which often requires the materials to be hydrophilic in nature. Implants that lack porosity typically do not integrate well with biological tissue, become fibrously encapsulated, and subsequently exhibit a higher risk of infection and expulsion.
This porosity should be hierarchical in nature and should span nano-, micro-,and millimeter length scales. With sufficient interconnected porosity and absorption qualities, implants of the correct compositions can rapidly vascularize, improving cell transport as well as nutrient and waste diffusion—ultimately ensuring that the implant can transform into viable living tissue. Interconnected porosity also has an added benefit of permitting a surgeon to preload the construct with patient bone marrow, antibiotics, growth factors, and other biological agents that could improve the patient outcome.
Although they exhibit biological advantages over metals, alloys, polymers, and composites thereof, ceramics are relatively difficult to form into complex structures with interconnected porosity suitable for biological ingrowth and integration. Further compounding this geometry challenge, every bone defect is unique, requiring each implant to be individually manufactured to directly fit the defect or be altered before or during surgery to fit the defect.
To address this forming and geometry challenge, two general approaches have been pursued: coating prefabricated and shaped metals, alloys, polymers, and composites with ceramics, and using additive manufacturing. Ceramic coatings greatly improve integration of metallic and polymeric implants, although the underlying implant does not transform into natural bone. For this reason, there have been significant efforts to additive manufacture ceramic-based biomaterials.
Additive manufacturing to capture form in ceramic-based biomaterials
The term “additive manufacturing” is broad in meaning and effectively covers any manufacturing process that is not subtractive in nature. However, the colloquial meaning of additive manufacturing is equated with 3D printing.
Medical 3D printing can be divided into three primary categories and multiple subcategories based upon the type of materials used and intended application of the end object (Figure 2). Briefly, traditional medical 3D printing focuses on production of surgical and training guides and models and permanent, nonregenerative implants.
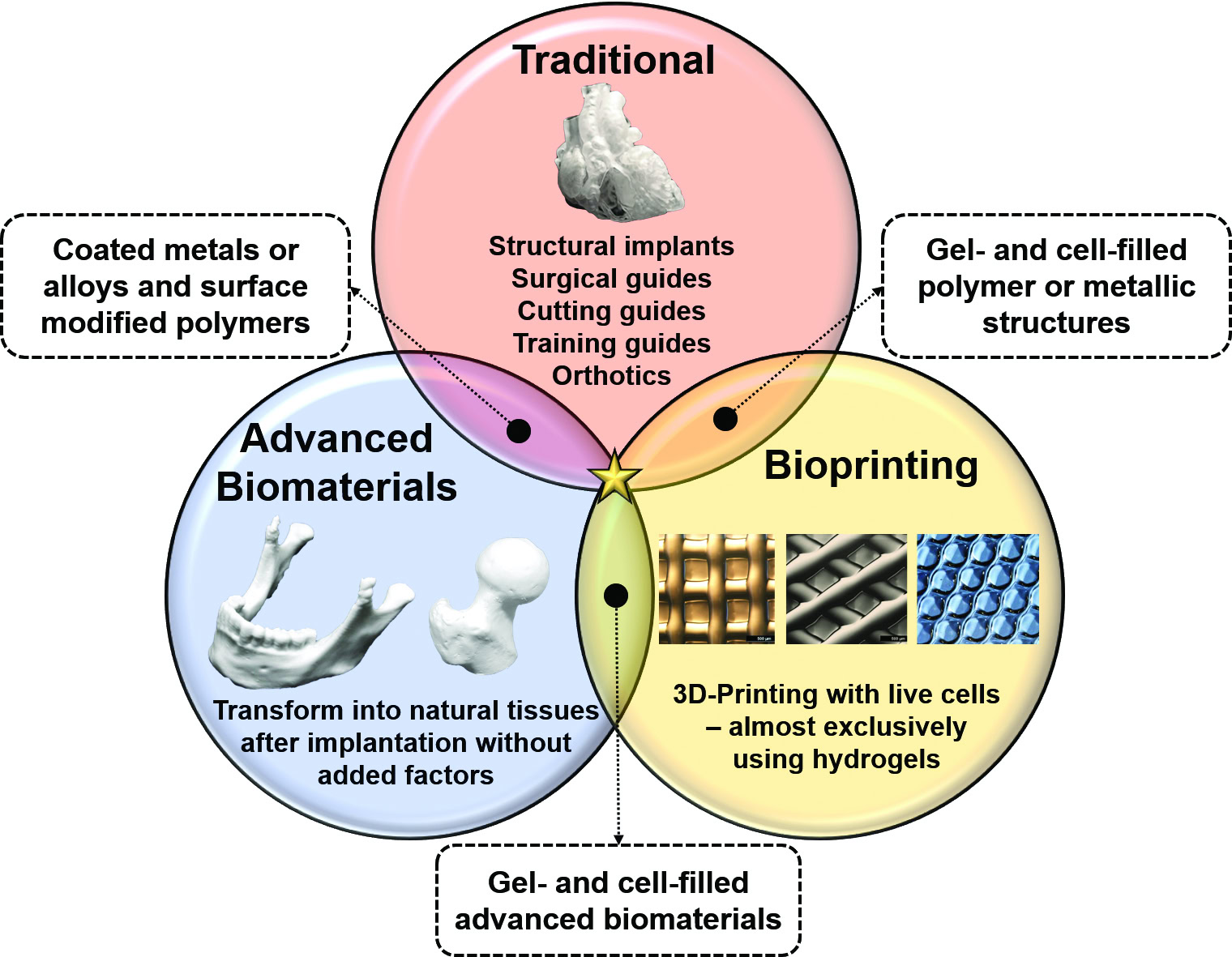
Figure 2. Three general types of medical additive manufacturing and their hybrids. Star represents technologies that marry biological tissue interfaces with nonbiological mechanics and electronics. Credit: Adam Jakus, PhD – Dimension inx
Bioprinting refers to any 3D printing process that uses living cells within the material as it is 3D-printed (not added after). Advanced biomaterial 3D printing includes emerging biomaterials, such as Hyperelastic Bone® (Dimension Inx, LLC; Chicago, Ill.), that are capable of independently inducing a strong regenerative response. More information on the three categories can be found in a book chapter by Jakus et al.5
Beyond the three medical 3D printing categories, there are six major 3D printing process technologies: fused deposition modeling (FDM), material extrusion, jetting, inkjet binding, powder-bed energy fusion, and resin-bath lithography.5 All of these technologies have been used to additively manufacture ceramics and their composites.
FDM deposits molten thermoplastics, such as polylactic acid (PLA) or polycaprolactone (PCL), which can be lightly loaded with ceramic powders, to create composite structures that are primarily polymer.
Material extrusion (nonthermal extrusion) processes are highly varied in nature, but traditionally use ceramic slurries suspended in water or an alcohol that are extruded to create green body structures, which are dried and sintered.
Inkjet binding uses ceramic powder beds and selectively deposits adhesives to generate green bodies layer-by-layer, which are cleaned of excess powders and then sintered.
Jetting processes use thermal or piezoelectric print heads to deposit ceramic-adhesive, liquid suspensions that are typically solidified via photo-crosslinking.
Powder bed fusion through selective application of thermal energy via laser or electron beam have also been used with some success to create complex ceramic parts, but the high sintering and melting temperatures of ceramics generally make the application of this approach more challenging and slower than metal or polymer counterparts.
Finally, stereolithographic methods can also be used to create complex, silicon-based ceramics (oxides and carbides) through thermal processing, decomposition, and sintering of polymeric objects formed through vat-polymerization of silicone-based resins.6
The end-user and clinical translation: surgical, economic, and regulatory considerations
What good is a new technology if the intended end-user cannot use it, does not want to use it, cannot afford to use it, and/or cannot access it? Beyond technical efficacy and ability to repair and regenerate bone, an ideal ceramic-based biomaterial must also be appealing to surgeons, cost-comparable or cost-reducing relative to other treatments/products, and cleared safe for human use by regulatory bodies, such as the United States Food and Drug Administration (FDA).
Broadly defined, surgical-friendliness refers to the quality of a product to be easily handled and surgically deployed into a biological defect site without complications or failure and without substantially extending overall surgery time. In any surgical procedure, limiting the amount of tissue that needs to be cut and exposed as well as limiting operation time is paramount.
Deploying a rigid, brittle object, such as a traditional sintered ceramic, into a complex boney defect not only requires maximum tissue exposure but also operating time. Additionally, native bone often must be moved, removed, shaped, and otherwise manipulated during surgery. Likewise, an implant must be modifiable to match the resulting defect geometry.
Traditional structural ceramics cannot be readily shaped, formed, or attached to native tissues without additional metallic hardware (plates and screws). Thus, even with ability to make complex, porous ceramic structures, existing ceramic-based biomaterial properties still suffer from this handling and shaping problem. An ideal ceramic-based biomaterial would not be brittle and could be trimmed, press-fit to complex voids, and sutured to surrounding tissues.
For a new technology and product to be translated, it must receive regulatory clearance, which is determined by the FDA in the U.S. The details of FDA medical device and biologic approval are beyond the scope of this article, but there are several important points. Contrary to common statements within the biomaterials research community, materials are not cleared by the FDA—products for specific applications (indications) are cleared.
This does not create any unique, additional challenge for additively manufactured products if all are standard shapes and sizes. In late 2017, the FDA released a guidance document on technical considerations for additive manufactured medical devices (available at fda.gov). An ideal ceramic-based biomaterial must also have clear regulatory clearance pathways.
Finally, while unfortunate, cost is king when it comes to most national healthcare systems as well as industries that manufacture and sell medical products. Surgeons, hospitals, and health systems are not likely to adopt a new product unless its cost is at least comparable with what is already in use.
From raw material availability and price to processing costs, manufacturing costs, regulatory clearance and maintenance costs, logistics and storage, packaging and sterilization, and profit margins on product sales, numerous factors combine to create a final unit price. Thus, an ideal ceramic-based biomaterial must be cost-effective relative to existing technologies.
3D-painting: a materials-centric approach to advanced manufacturing
Keeping these technical, manufacturing, surgical, regulatory, and economic considerations in mind, it might seem impractical if not impossible to create a ceramic-based biomaterial that addresses all these needs while also being compatible with 3D printing and capable of being implemented to create additional generations of TERM products and multimaterial TERM products that can address multiple tissues.
To address these needs, Ramille N. Shah and I created a 3D-painting materials manufacturing technology platform and ceramic-based composite called Hyperelastic Bone. Initially demonstrated in 2012, first published in 2016,7 made commercially available through Dimension Inx in 2017, and currently progressing toward clinical use, 3D-painted Hyperelastic Bone and its variants represent a distinct approach to ceramic-based biomaterials that fulfil the necessary criteria of a translationally effective bone biomaterial.
3D-painting is a materials-centric advanced manufacturing technology that permits nearly any material to be transformed into a 3D-printable “3D-paint” via simple, room-temperature extrusion without the need for support materials, powder-beds, resin-baths, cross-linking, or curing. 3D-paint materials developed to date include biological decellularized extracellular matrices,8 ceramics,9 metals and alloys,10 graphene,11 and advanced polymers.12 A full list of 3D-paints is available at dimensioninx.com, as well as additional 3D-painting related publications.
All 3D-paints are co-3D-printing compatible with each other (multimaterial fabrication) and can be mixed or blended prior to or during 3D printing to create compound 3D-paints comprising multiple distinct base materials.
Compatible with existing bioprinter platforms (simple x–y–z extruders) and modified FDM platforms, 3D-paints are analogous to common paints in terms of major components, but they dry or solidify substantially faster. Upon extrusion from a nozzle, 3D-paint rapidly solidifies via near-instantaneous evaporation of the evaporant while also being able to chemically weld with previously deposited materials.
3D-painted Hyperelastic Bone: changing the way we think of ceramic-based biomaterials
Although more than 100 3D-paints have been developed to date, Hyperelastic Bone represents a singular 3D-paint specifically engineered for bone repair and regeneration applications.7 Like all 3D-paints, Hyperelastic Bone can be rapidly 3D-printed at room-temperature into simple or complex forms, extruded into fibers, and subsequently braided or woven into textiles, cast into sheets, and more (Figure 3).
3D-painted Hyperelastic Bone is comprised of 90 wt.% calcium phosphate ceramic microparticles linked by a matrix of 10 wt.% high-quality, medical grade, biodegradable elastomer. Because the elastomer binder component of Hyperelastic Bone is medical-grade, biocompatible, bioresorbable, and manufactured specifically for medical implants, 3D-painted Hyperelastic Bone structures do not need thermal processing and, consequently, do not need to be sintered to yield stable ceramic-based structures. 3D-painted objects only need to be washed and sterilized prior to biological use.
The composition and microstructure of 3D-painted Hyperelastic Bone are so similar to natural bone that resulting computed tomography reconstructions of 3D-painted Hyperelastic Bone parts are difficult to distinguish from natural bone (Figure 3).
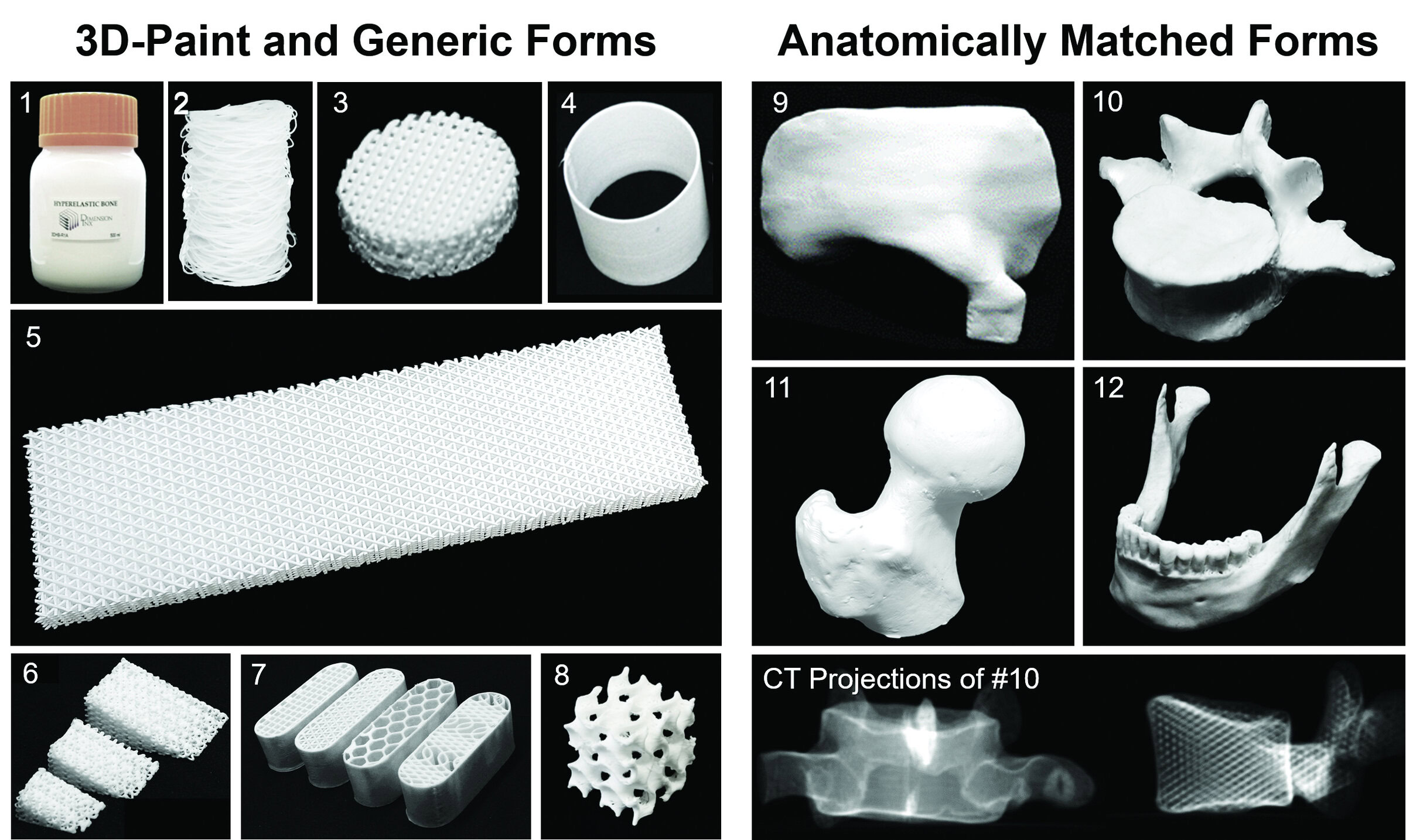
Figure 3. Hyperelastic Bone 3D-paint (1) and extruded fiber (2) can generate various generic 3D-painted forms (3–8) and forms based on patient 3D imaging data, including partial skull and orbital bone (9), lumbar vertebra (10), femoral head (11), and mandible and teeth (12). Bottom right panel shows projections of computed tomography (CT) reconstruction of lumbar vertebra from panel 10, which demonstrates imaging signature of 3D-painted Hyperelastic Bone and its similarity to natural bone. Credit: Adam Jakus, PhD – Dimension inx
The ceramic-elastomer composite matrix microstructure is characterized by interconnected micro- and nanoporosity, producing a total microstructural porosity of up to 50 percent—imparting advantageous mechanical and handling properties and liquid absorption (wicking) characteristics (Figure 4).
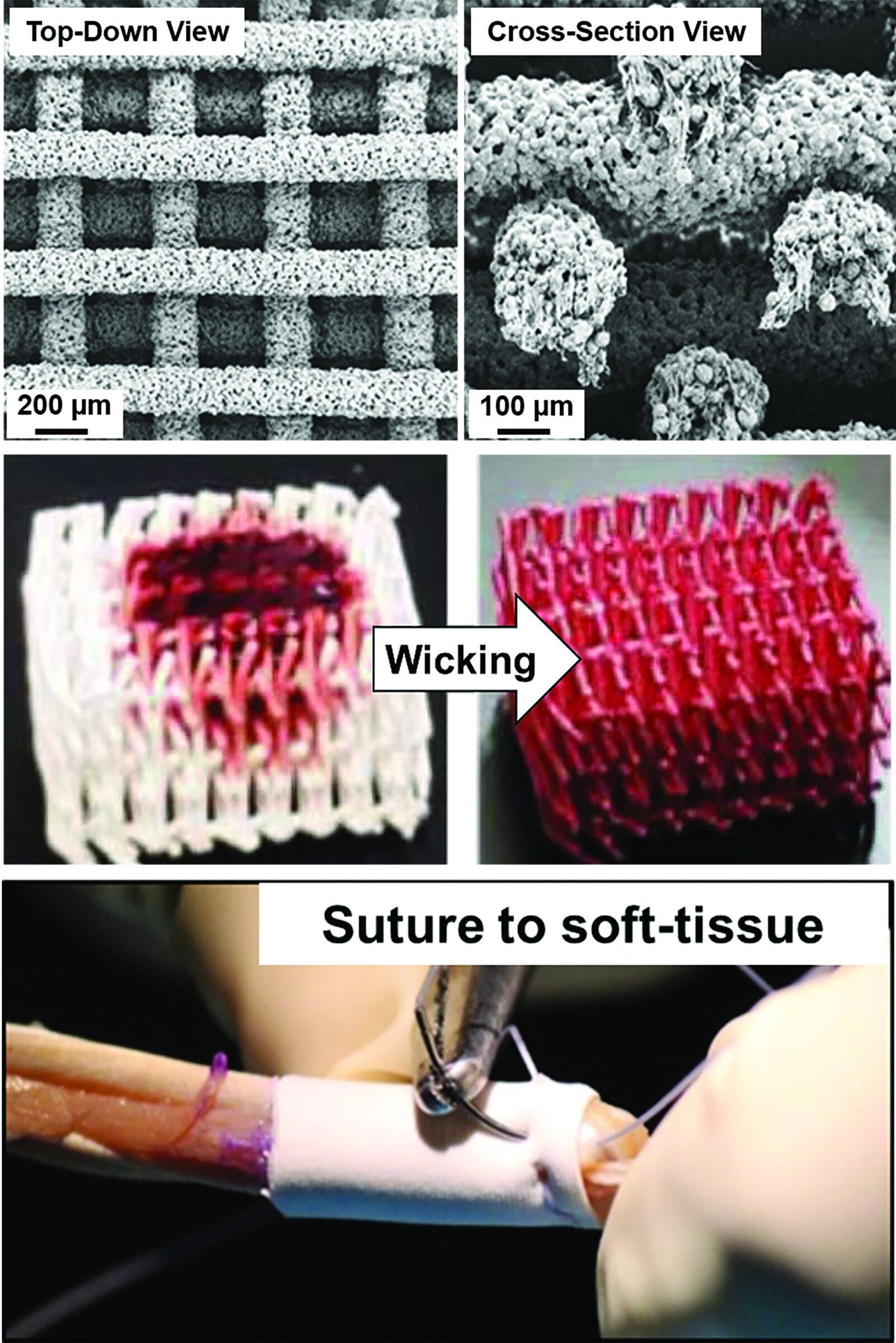
Figure 4. (Top) Scanning electron micrographs of 3D-painted Hyperelastic Bone scaffold, highlighting micro- to nanoporosity within the material and linking of discrete ceramic particles by elastomer. (Bottom) Photographs of Hyperelastic Bone absorbing and distributing viscous liquid throughout its volume. Credit: Adam Jakus, PhD – Dimension inx
With such high ceramic content—20–30 percent higher than natural bone—one might expect Hyperelastic Bone to be brittle and ultimately unsuitable for surgical use. However, its unique composition and architecture of rigid ceramic particles linked by elastomer bridges and surrounded by substantial porosity results in elastic-like and macroscopically observable mechanical properties, which is of great interest to surgeons.
Hyperelastic Bone essentially acts as a flexible bioceramic capable of being cut, rolled, folded, press-fit into complex boney defects, and even sutured to biological tissues for fixation (Figure 4)—all characteristics that are ideal for surgical applications to treat complex, irregularly shaped boney defects.
Biologically, Hyperelastic Bone has been demonstrated over the past seven to eight years to be highly bioactive and osteoregenerative in both in vitro and in vivo studies (Figure 5).
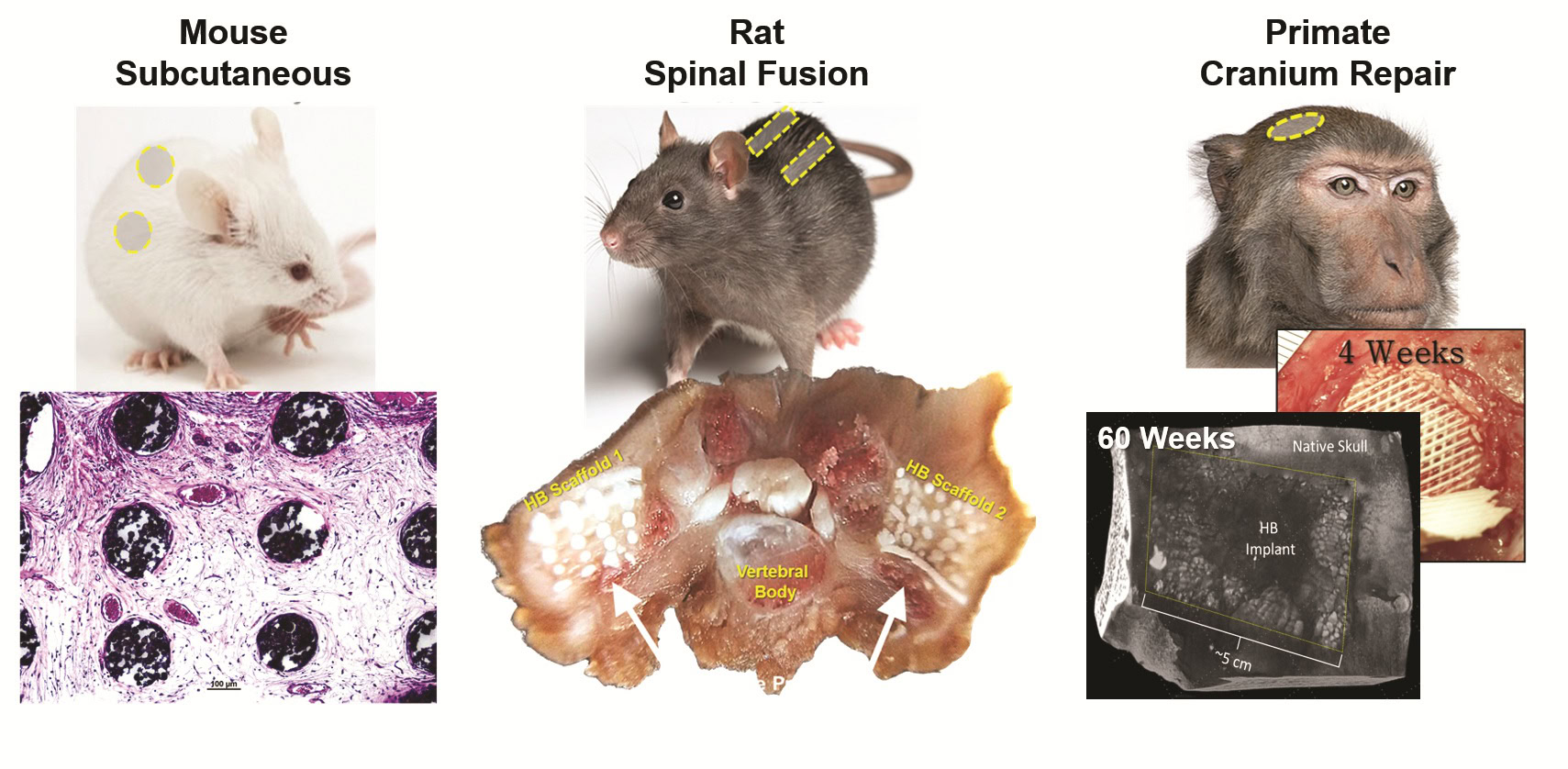
Figure 5. Selected in vivo studies have examined safety and efficacy of Hyperelastic Bone, including mouse subcutaneous implant, rat posterolateral spinal fusion, and Rhesus macaque large segmental cranium repair. Credit: Adam Jakus, PhD – Dimension inx
3D-painted Hyperelastic Bone scaffolds not only support adult stem cell attachment and proliferation but also stem cell differentiation to osteoblast-like (bone-producing) cells without the need for added growth factors or chemical or mechanical stimuli.7 Additional studies show that Hyperelastic Bone scaffolds support attachment, proliferation, and alignment of human umbilical vein endothelial cells, which are primarily responsible for forming vessels and vasculature.13
Hyperelastic Bone also has been extensively used in various 3D-painted forms in numerous animal models for implant periods ranging from several weeks to 15 months. Hyperelastic Bone scaffolds implanted under the skin of mice for up to seven weeks rapidly integrate with tissues and form blood vessels, without eliciting a significant immunological response.7
In rat spine fusion models, Hyperelastic Bone scaffolds promote boney ingrowth and fusion, with results similar to allograft demineralized bone matrix. In large primates with full-thickness cranial defects, 3D-painted Hyperelastic Bone sandwich laminate structures (solid top and bottom with porous interior) up to 5 cm in length that are surgically shaped intraoperatively to fit the complex boney void rapidly vascularize and integrate with surrounding tissue after four weeks, and they remain stable and show full boney regeneration and integration at 15 months.7
Beyond technical and surgical benefits of 3D-painted Hyperelastic Bone, the material is also compatible with cost-effective, advanced manufacturing and appears to be economically viable. With respect to raw materials, Hyperelastic Bone 3D-paint and corresponding 3D-painted structures are comprised of purely synthetic, mass-manufactured, high-quality materials already in widespread clinical use.
3D-paints can be rapidly synthesized in small (<5 mL) or large (multiliter) batches, are chemically stable, and can be 3D-printed at rapid speeds with any extrusion-based printing hardware. Combined, these factors indicate that, even after regulatory approval processes, 3D-painted Hyperelastic Bone products could be cost-competitive with contemporary, less efficacious bone grafting products in clinical use.
Beyond the structural, biological, handling, manufacturing, and economic advantage of Hyperelastic Bone, its current form offers many future opportunities for ceramic-based 3D-painted products that take advantage of the unique nature of 3D-painting technologies. One such advantage is compositional versatility. Because the 3D-painting process is primarily chemistry-independent, many distinct types of ceramics and even glasses can be used to create 3D-paints and 3D-painted structures.
“Classic” Hyperelastic Bone is based on hydroxyapatite, but 3D-paints comprised of the previously mentioned ceramics have all been demonstrated. Further, additional agents, such as antibiotics, small molecules, peptides, proteins, or nanoparticles, can be directly incorporated into 3D-paints prior to 3D-painting. 3D-painted Hyperelastic Bone and other 3D-painted biomaterials can also act as effective carriers for cells, hydrogels, and more.
The near future of 3D-printed ceramic-based biomaterials
Due to extensive understanding of the benefits and deficiencies of existing ceramic-based biomaterials, targeted engineering and surgeon-guided development, and application of materials science principals, Hyperelastic Bone has come a long way in just the past several years. Although not yet FDA cleared, the rapid progression of Hyperelastic Bone demonstrates that there is a clear clinical need and medical desire for ceramic-based biomaterials for bone repair and regeneration.
At the same time, Hyperelastic Bone represents a singular composition from the 3D-painting materials platform technology, which permits near-endless versatility and room to explore musculoskeletal tissue repair and regeneration. However, as development continues to progress, one must consider not only technical criteria, but also the end-user (i.e., surgeons) and reality of cost in medicine.
Ceramic-based biomaterials will continue to play a key role in tissue engineering and regenerative medicine, but that role is still part of a much larger story that will require knowledge and integration of extremely diverse materials to repair, regenerate, and replace the complex materials that make us human.
Capsule summary
Age of advanced biomaterials
Recent convergence of the fields of medicine and materials science and engineering—combined with advanced manufacturing techniques—may usher in a new age of advanced biomaterials to dynamically repair human tissues.
Ceramic solutions
Ceramic-based biomaterials offer structural, biological, handling, manufacturing, and economic advantages that make the materials well-suited for tissue repair and regeneration. Emerging ceramic-based biomaterials that also are compatible with additive manufacturing and clinically suitable may enable entirely new directions.
Adding up to a new future
Together, a new additive materials platform technology and ceramic-based biomaterials permit extensive versatility to explore musculoskeletal tissue repair and regeneration. However, continued development must consider not only technical criteria, but also the end-user and reality of medical costs.


Related Articles

Market Insights
Engineered ceramics support the past, present, and future of aerospace ambitions
Engineered ceramics play key roles in aerospace applications, from structural components to protective coatings that can withstand the high-temperature, reactive environments. Perhaps the earliest success of ceramics in aerospace applications was the use of yttria-stabilized zirconia (YSZ) as thermal barrier coatings (TBCs) on nickel-based superalloys for turbine engine applications. These…

Market Insights
Aerospace ceramics: Global markets to 2029
The global market for aerospace ceramics was valued at $5.3 billion in 2023 and is expected to grow at a compound annual growth rate (CAGR) of 8.0% to reach $8.2 billion by the end of 2029. According to the International Energy Agency, the aviation industry was responsible for 2.5% of…

Market Insights
Innovations in access and technology secure clean water around the world
Food, water, and shelter—the basic necessities of life—are scarce for millions of people around the world. Yet even when these resources are technically obtainable, they may not be available in a format that supports healthy living. Approximately 115 million people worldwide depend on untreated surface water for their daily needs,…