
The main body of research involving bioactive glasses (BGs) has been devoted to applications in orthopedics and dentistry, given that the original composition 45S5 Bioglass™ was developed to treat non-self-healing bone defects, such as bullet trauma or cancer.1,2 Because of their high bioactivity, BGs directly bond to bone. That bioactivity recently has been appreciated to extend to interaction with soft tissues as well.3,4 Many of the cellular processes involved in the early stages of soft tissue regeneration are affected by ionic dissolution products released by BGs, and an important aspect of BG applications in soft tissue repair strategies is their angiogenic potential.
Surface reactions of BGs in contact with relevant fluids—which result in release of metallic ions (depending on BG composition) and precipitation of a hydroxyapatite (HA) surface layer—have been studied extensively.5,6 Several BG formulations also exhibit antibacterial effects and, therefore, lead to successful clinical outcomes, for example, to combat osteomyelitis.7 The therapeutic effect of metallic ions added to BGs on osteoblast cells has been established as highly beneficial in the context of bone regeneration, especially given gene upregulation in osteoblast cells, increased extracellular matrix mineralization, and proliferation of osteoblasts occur in the presence of specific concentrations of BG dissolution products.8
Research into the application of BGs in soft tissue engineering has delved into areas such as peripheral nerve repair9 and chronic wound healing.10 Other tissues also are being considered, which are summarized in Figure 1 and have been discussed in recent literature.3,4 This article compiles the most recent publications in the field to provide a concise overview of the suitability and potential of BGs in soft tissue engineering. While highlighting the angiogenic effect of BGs, we also focus on wound healing and nerve regeneration.
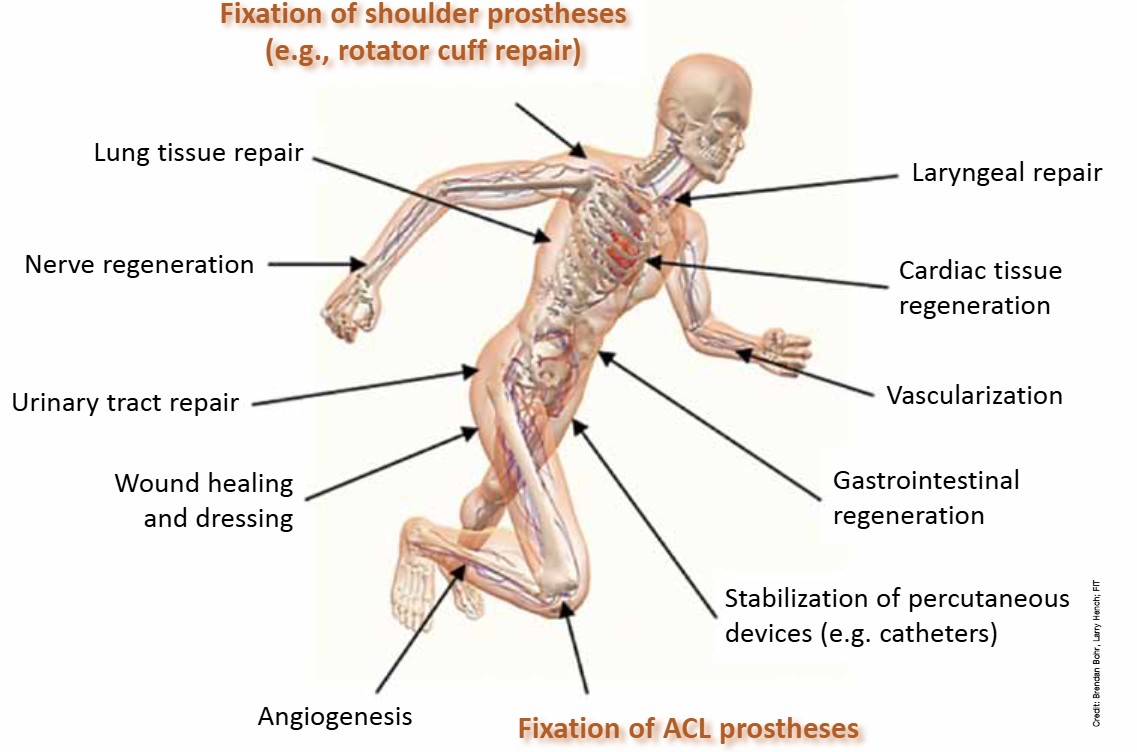
Figure 1. Potential applications of bioactive glasses in contact with various soft tissues currently being investigated. Applications involving fixation of ACL and shoulder prostheses are included for completeness, although they are not discussed in this article. Credit: Brendan Bohr, Larry Hench; FIT
Angiogenesis
Angiogenesis is a crucial process that takes place in normal tissue regeneration and repair as well as in some pathogenic processes, such as cancer. Angiogenesis involves sprouting of new blood vessels from existing ones, a process carefully orchestrated and driven by mechanical stress and chemical cues—chiefly growth factors, extracellular matrix proteins, and other signalling molecules—produced by cells in surrounding tissues. Angiogenesis is a crucial step in any tissue-engineering strategy, because new tissue requires adequate oxygenation and mass transport to and from cells.
One approach to stimulate angiogenesis in tissue-engineering constructs is the direct introduction of growth factors and signalling molecules onto constructs’ surfaces. However, production and isolation of these angiogenic factors is expensive, and their release kinetics and efficiency of delivery to surrounding tissues once implanted remain incompletely understood. In addition, manufacturing methods or necessary pretreatments of tissue-engineering scaffolds may alter or damage the 3-D structure of these bioactive molecules, thus rendering them inadequate. For these and other reasons, i.e., costs, alternative methods of promoting angiogenesis—especially those where the scaffold material’s degradation products act themselves as stimulants of this process—are needed.
There is substantial in-vivo and in-vitro evidence that BG dissolution products have an angiogenic effect.11 In particular, direct stimulation by BG dissolution products produces relevant growth factors, namely vascular endothelial growth factor (VEGF) and basic fibroblastic growth factor (bFGF) in fibroblast cells. A recent article12 discusses individual metallic elements and their role in angiogenesis, although effects that may occur in in-vitro and in-vivo experiments involving BGs will most likely be caused by the combined action of various released ions. Further research is required to investigate individual effects of metallic ions released by BGs and the effect of specific ratios of ion concentrations. Also, increased pH associated with the dissolution–precipitation of BGs in relevant solutions affects cell processes and correlates with increased metabolic activity and proliferation rate in mammalian cells.13
Many publications report research on the angiogenic effects of BGs in the context of bone tissue engineering.11 Recently, El-Gendy et al.14 studied the angiogenic effect of 45S5-Bioglass-based scaffolds and human dental pulp cells for tissue-engineered bone constructs. The study found increased endothelial gene expression in cells seeded onto 3-D porous scaffolds in-vitro and formation of microvessel-like tubular structures eight weeks after implantation in male immunocompromised mice.
Of relevance for the application of BGs in soft tissue repair, where vascularization is a prerequisite, previous work examined the effects of culturing human umbilical vein endothelial cells (HUVECs) with extracts of nanosized 58S and 80S BGs (58S-NBG and 80S-NBG, respectively), which are sol–gel-derived, mesoporous BGs.15 That study assessed angiogenic effects using an extracellular matrix gel tube formation assay and following mRNA expression of five angiogenic-related gene markers. Extracts from BG formulations stimulated proliferation and migration of HUVECS and production of VEGF and bFGF, and upregulated expression of their respective receptors together with those for nitric oxide synthase, which is also believed to be a key angiogenic marker.
These results complement a previous study conducted with human fibroblasts, which also demonstrates the pro-angiogenic effects of BGs. That study examined angiogenic markers from human fibroblast cells (CCD-18Co) encapsulated in alginate beads containing 45S5 BG particles ranging from 0% to 1% (w/v).16 Incubating beads with 0.01% and 0.1% (w/v) 45S5 BG content in culture medium for up to 17 d stimulated increased secretion of VEGF. In addition, culture medium containing exudates from alginate beads containing 0.1% (w/v) 45S5 BG stimulated proliferation of human dermal microvascular endothelial cells (HDMECAs) in-vitro.
Boron-doped 45S5 BG (45S5.2B) has also been studied recently for its angiogenic effect using an embryonic quail choroallantoic membrane model, which showed that the BG’s ionic dissolution products stimulated angiogenesis.17
The results of these studies compound previous investigations that found various compositions of BGs stimulate angiogenic growth factor production in-vitro and provide interesting avenues for neovascularization of tissue-engineering constructs. Since publication in 2010 of the first review article summarizing angiogenic evidence of BGs, many studies have been published (detected using keywords “vascularization” or “angiogenesis” combined with “bioactive glass” in publication databases), adding in-vitro and in-vivo evidence to this field.
Wound healing
In clinical scenarios of extensive skin damage caused by injury or disease or nonhealing wounds, such as diabetic skin ulcers, considerable care is needed to simultaneously restore damaged tissue, avoid infection, and remove excessive tissue exudates that might impair adequate healing. Nanofibrous BG dressings and ointments containing BG particles of various compositions have found success in clinical and animal studies, respectively, to accelerate wound healing and improve the quality of newly formed tissue. In the case of dressings, BG nanofibers provide cellular mechanical support and a source of therapeutic ions, aiding tissue regeneration as demonstrated for borate glass fibers.10
Recent investigations have examined in-vitro degradation and HA deposition of BG nanofibers and microfibers of 45S5, 13-93B3, and 1605 (doped with CuO and ZnO) compositions (Table 1) in static and dynamic-flow models.18 BG compositions 13-93B3 and 1605 exhibit faster ion release and glass conversion compared with 45S5 BG, and trace amounts of added elements (namely copper and zinc) influence fiber bioactivity. Further, experiments with CCL-110 human skin fibroblast cells show that presoaking fibers in culture medium or providing an adequate medium flow rate benefit cell migration and proliferation.
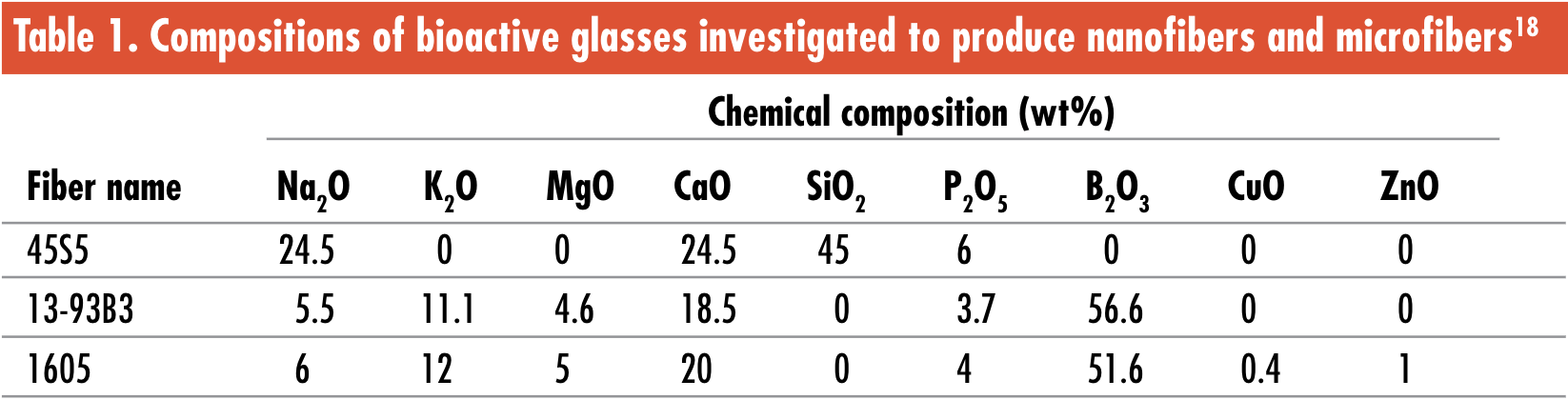
Credit: Compositions of bioactive glasses investigated to produce nanofibers and microfibers graphic created by ACerS using data from Reference 18.
In a similar recent study, Zhao et al.19 investigated the utility of copper-doped borate BG (CuB–BG) microfibers as wound dressings in-vitro and in-vivo. CuB-BGs doped with 0–3.0-wt% CuO were converted into HA after only 7 d of immersion in simulated body fluid in-vitro. In addition, treatment of HUVEC cell cultures with only BG fiber culture supernatants can promote cell migration, tubule formation, and production of VEGF, whereas culture with human primary dermal fibroblasts upregulates angiogenic-related gene expression. Microfiber dressings of 3.0-wt% CuO CuB–BG fibers increase stimulation of angiogenesis in full-thickness skin defects in rodents. Doped and undoped fibers markedly improve wound tissue healing through collagen fiber deposition, orientation, and maturity compared with untreated controls at 7- and 14-d post-operation. At 14 d, defects treated with doped or undoped fibers exhibit no significant difference in tissue quality.
A setup used by Ma et al.20 produced nanofibrous BG (composition (wt%): 30 SiO2, 27 CaO, 20 B2O3, 4 P2O5, 1.5 CuO, 1 ZnO, 3 K2O, and 9 Na2O) and gelatin/chitosan (G/C) composite membranes for use in chronic wound management by electrospinning. Pure G/C and composite G/C with 15-wt% BG membranes implanted subcutaneously into surgical incisions mimicking wounds degraded after four weeks, with no inflammation in surrounding tissues. Altogether these results demonstrate that BGs, especially various compositions in fibrous morphologies, are excellent options for wound-healing applications, because they mediate cell migration and proliferation based on their capacity to stimulate angiogenesis.
Nerve regeneration
Scission or other damage to peripheral nerves normally elicits a regenerative response by the body, but depending on the degree of damage and size of the injury, full recovery of motor and sensory functions may not occur. The use of implants to aid nerve regeneration has focused mainly on bridging gaps left by sectioning damaged tissue and have been made using natural and synthetic polymeric materials. However, in an increasing number of studies, the application of BGs and particularly fibrous BGs is leading to more promising results.
Olfactory ensheathing cells (OECs) aid nerve regeneration in the olfactory system and the rest of the central nervous system and are involved in axon myelination.21 As such, this cell type has potential use in nerve regeneration. A recent study by Renno et al.22 exposed OECs—seeded on biosilicate (a bioactive glass-ceramic (BGC) of the quaternary Na2O–CaO–SiO2–P2O5 system) disks and collagen scaffolds—to single laser irradiation at 830 nm under the supposition that it would speed up OEC growth and proliferation. OECs cultured for up to three weeks successfully grew on both substrates. However, laser-irradiation increased cell population on collagen scaffolds and decreased cell population on BGC disks. The study’s authors speculate that interaction of the laser with BGC’s crystalline structure may inhibit OEC proliferation, although further investigation is needed to confirm that speculation. In any case, the successful seeding and incubation methods of this study may be of use in future research involving BGs and OECs.
Another recent study by Moham-madkhan et al.23 developed poly-(ε)-caprolactone (PCL) and BG composite sheets as flexible biomaterials for neural tissue engineering. Specifically, composite sheets were fabricated with 50-wt% PCL and 50-wt% 13-93 B3 BG, 50-wt% 45S5 BG, or 25-wt% each 13-93 B3 and 45S5 BG particles. Sheets cultured with embryonic chicken dorsal root ganglia cells for up to 72 h stimulated neurite outgrowth on as-fabricated 45S5 and pretreated 13-93 B3 composites compared with pure PCL controls, confirming that BG-containing composites are promising nerve guide conduit materials.
Recently, the cytocompatibility of silica-based BGs containing Y2O3 and CeO2 was tested by Placek et al.24 by incubating murine fibroblast and osteoblast cells with BG extracts. BG extracts exhibited good cytocompatibility, and the authors suggest that these BGs would be suitable candidates for nerve regeneration, because the inclusion of yttrium and cerium in the compositions may impart antioxidant effects, thus reducing damage to surrounding nerve tissues caused by oxidative stress experienced after trauma.
Bonding mechanisms between BG and soft tissues
The mechanism of bonding between BGs and soft and hard tissues is governed by well-established dissolution and precipitation reactions that occur at BG surfaces upon contact with physiological fluids.2,8,25 A local pH increase caused by increased concentration of various ions at the BG–fluid interface results in formation of a carbonated HA layer at the interface. This crystalline layer provides a bonding interface between implant and tissue. Two types of interactions occur in the body upon implantation of BGs,8,26 as summarized in Table 2 and Figure 2.
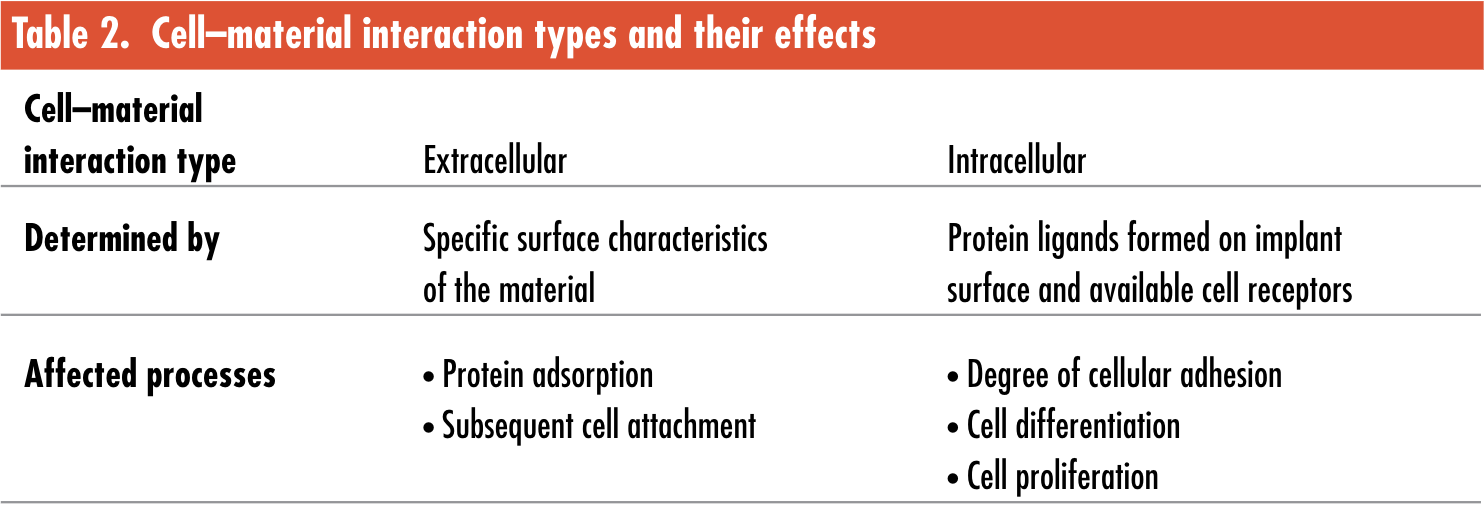
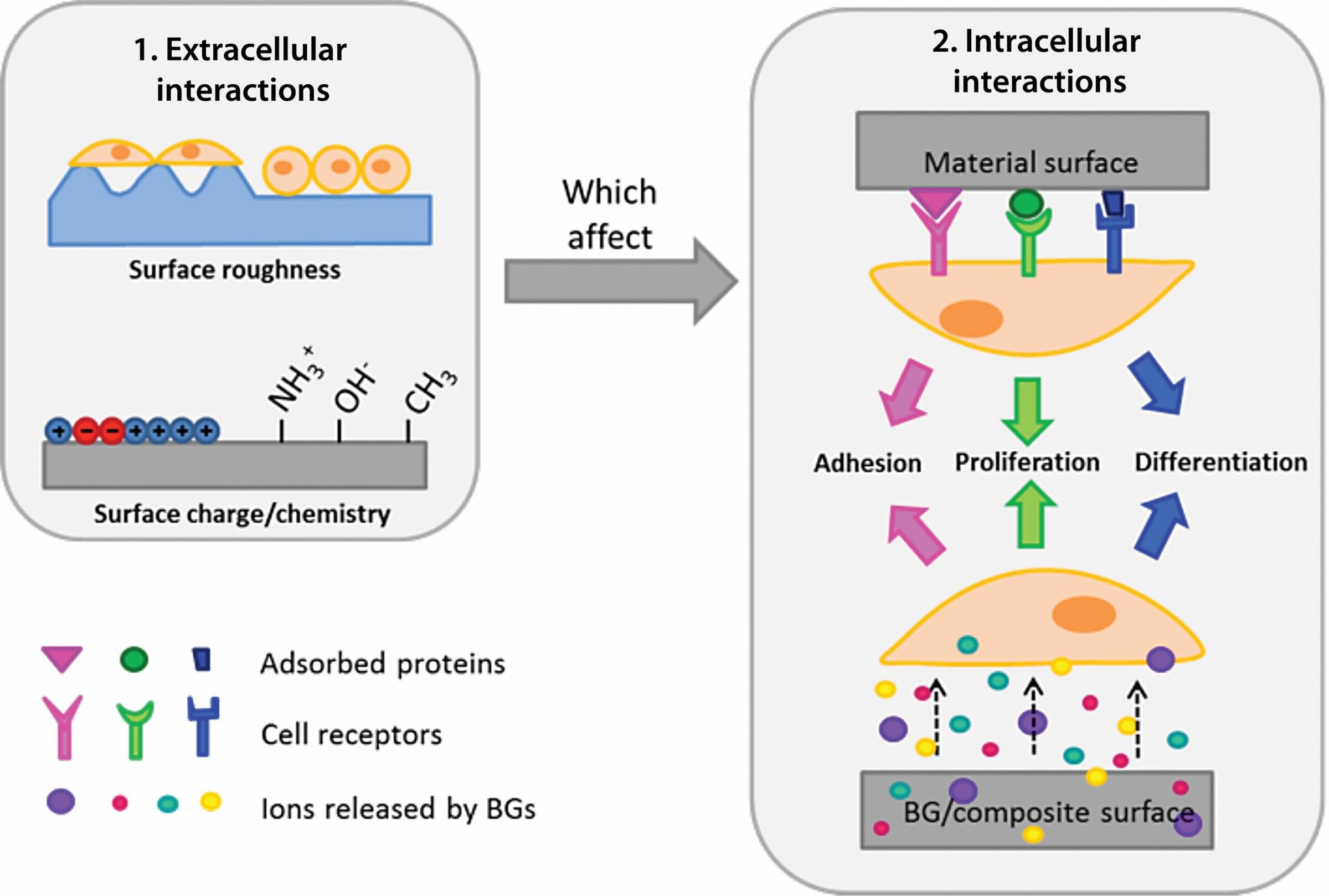
Figure 2. Types of material surface characteristics and how they affect cellular processes. Credit: Valentina Miguez-Pacheco; U. of Erlangen-Nuremberg
Of particular importance for BGs, these two types of interactions are affected by the availability of various ions and, thus, are highly dependent on specific BG composition. Additionally, collagenous constituents of soft tissues can attach to BG surfaces, although bonding and rate of regeneration are partially dependent on progenitor cell populations available in surrounding tissues.27 Although there is evidence that BGs can attach to various soft tissues, the mechanisms responsible for these observations have not been fully described, and, therefore, this remains an area of active research.
Biomechanical aspects
Clinical applications of BGs in contact with soft tissues have two primary requirements for success:
- Rapid formation of an interfacial layer mediated by extracellular matrix molecules; and
- Stable long-term interfacial bonding that prevents micromotion at the interface and inflammatory responses.
The excellent long-term clinical success of 45S5 BG devices for replacement of bones of the middle ear and implants for maintenance of edentulous jaws (ERMIs), reviewed by Hench and Greenspan,27 are attributed to satisfying the above requirements for bone and soft connective tissues. Stable bonding of the implant to soft tissues prevents extrusion of ossicular replacements through the tympanic membrane or exfoliation through gingival tissues.
An early canine study by Wilson et al.,28 using the same ERMI implants, burs, and protocols as for humans, made it possible to achieve a quantitative histo-morphometric analysis of the hard and soft tissue bonding interfaces of ERMIs. Within three months, bonding stabilized for hard and soft tissues. Soft tissue was bonded by collagen fibers interdigitated within a 150–400-μm-thick bonding gel layer composed of biological HCA and an underlying silica-rich gel layer that began to form on implants within minutes of implantation. It was proposed that the difference in Young’s modulus in the interfacial area between soft tissue and bulk BG implant is spread over a substantial interfacial thickness because of an elastically compliant hydrated silica gel (HCA) layer on the BG, which is several hundred micrometers thick.27 Rapid formation of the bonding layer, as well as low stiffness of this bonding zone and the favorable stress transfer resulting from bonding of collagen fibrils, was concluded to be responsible for short- and long-term success of 45S5 Bioglass ERMIs.28,29
Conclusions
Available literature on the interactions of BGs and soft tissues unequivocally points to high suitability of BG materials for a range of applications beyond traditional areas in orthopedics and dentistry. The relative ease of manufacture and low cost of producing BGs of various chemical compositions in particulate, fibrous, mesoporous, or macroporous 3-D forms—whether the BG is intended for use alone or as part of a composite—make these materials highly attractive for clinical applications. The wide range of compositions studied (not considering those yet to be discovered) allow tailored therapeutic ion release and delivery according to the tissue type and conditions to be repaired, thus bringing an expanding range of options and opportunities for applications of BGs in soft tissue repair. The soft tissue bonding ability of BGs and their proven bioactivity and angiogenic abilities suggest that it is only a matter of time before BGs are more broadly exploited in a wide range of soft tissue applications that were unthinkable a few years ago.
The research discussed above indicates that BGs offer the potential to achieve regeneration of all connective tissues. Control of the rate of release of ionic stimuli by composition and surface area of BG formulations makes it possible to synchronize surface reaction kinetics with various cells and stimulate differentiation towards the mature phenotype required to regenerate anisotropic 3-D tissues with a complex extracellular matrix. Understanding genetic upregulation and activation by ionic stimuli released from BGs offers the possibility of developing patient-specific therapies, a huge challenge for the aging population.
Capsule summary
Background
Bioactive glasses were originally developed to treat non-self-healing bone defects, and they have been developed into various successful clinical applications for orthopedics and dentistry.
New uses
The properties of bioactive glasses and how they interact with biological systems also makes the materials of interest for soft tissue repair strategies.
Looking forward
Available literature indicates that the soft tissue bonding ability of bioactive glasses and their proven bioactivity and angiogenic abilities make the materials suitable for a range of soft tissue applications that were unthinkable a few years ago.

Related Articles

Bulletin Features
Emerging Professionals: Science for Society & Future Focus
Science for Society articles: Rishabh Kundu and Ryan C. Eaton: “One small tweak to the lens of materials research, one giant leap for mankind” Grace Dunham: “Microwave firing: Inspiring young scientists through rapid ceramic demos” Hossein Libre: “Shaping materials science through policy engagement” Future Focus articles: Kartik Nemani: “Hope and…

Bulletin Features
Emerging Professionals: Research Articles
Experiential learning: Developing the next generation of engineers By Ryan Eaton When a measure becomes a target, it ceases to be a good measure. Goodhart’s law, coined in reference to monetary policy, is readily applicable to engineering education. When students begin optimizing their study habits to pass an exam rather…
Bulletin Features
Durable and programmable metasurfaces enabled by phase change materials
Controlling light with high spatial precision enables technologies ranging from imaging and sensing to communications. Traditionally, optical components such as lenses and filters rely on bulk materials and fixed geometries, which limit their ability to adapt dynamically. Metasurfaces offer a fundamentally different approach. These materials consist of planar arrays of…